What is a nonverbal learning disorder? Tim Walz’s son Gus’ condition, explained
Gus Walz stole the show Wednesday when his father, Minnesota Gov. Tim Walz, officially accepted the vice presidential nomination on the third night of the Democratic National Convention.
The 17-year-old stood up during his father’s speech and said, “That’s my dad,” later adding, “I love you, Dad.”
The governor and his wife, Gwen Walz, revealed in a People interview that their son was diagnosed with nonverbal learning disability as a teenager.
A 2020 study estimated that as many as 2.9 million children and adolescents in North America have nonverbal learning disability, or NVLD, which affects a person’s spatial-visual skills.
The number of people who receive a diagnosis is likely much smaller than those living with the disability, said Santhosh Girirajan, the T. Ming Chu professor of biochemistry and molecular biology and professor of genomics at Penn State.
“These individuals are very intelligent and articulate well verbally, but they are typically clumsy with motor and spatial coordination,” he told NBC News. “It’s called a learning disorder because there are a lot of cues other than verbal cues that are necessary for us to keep information in our memory.”
People with NVLD often struggle with visual-spatial skills, such as reading a map, following directions, identifying mathematical patterns, remembering how to navigate spaces or fitting blocks together. Social situations can also be difficult.
“Body language and some of the things we think about with day-to-day social norms, they may not be able to catch those,” Girirajan said.
Unlike other learning disabilities such as dyslexia, signs of the disability typically don't become apparent until adolescence.
Early in elementary school, learning is focused largely on memorization — learning words or performing straightforward mathematical equations, at which people with NVLD typically excel. Social skills are also more concrete, such as playing a game of tag at recess.
“But as you get older, there’s a lot more subtlety, like sarcasm, that you have to understand in social interactions, that these kids might not understand,” said Laura Phillips, senior director and senior neuropsychologist of the Learning and Development Center at the Child Mind Institute, a nonprofit organization in New York.
In her own practice, she typically sees adolescents with NVLD, who usually have an average or above average IQ, when school demands more integrated knowledge and executive functioning, such as reading comprehension or integrating learning between subjects. They also usually seek help for something else, usually anxiety or depression, which are common among people with NVLD.


Sometimes misdiagnosed as autism
Amy Margolis, director of the Environment, Brain, and Behavior Lab at Columbia University, is part of a group of researchers that is beginning to call the disability “developmental visual-spatial disorder” in an effort to better describe how it affects people who have it.
People with NVLD are “very much verbal,” Margolis said, contrary to what the name suggests.
The learning disability is sometimes misdiagnosed as autism spectrum disorder. Margolis led a 2019 study that found that although kids with autism spectrum disorder and NVLD often have overlapping traits, the underlying neurobiology — that is, what’s happening in their brains to cause these traits — is unique between the two conditions.
Margolis is trying to get NVLD recognized by the DSM-5, the handbook health care providers use to diagnose mental health conditions. Without such official recognition, people with NVLD can struggle to get the resources they need, such as special class placements or extra support in school.
“Without an officially recognized diagnosis, it’s hard for parents to understand how to seek information, and then communicate to other people what kinds of things might be challenging for their kid,” Phillips said, adding that widespread awareness is key to helping these families navigate NVLD.
Kaitlin Sullivan is a contributor for NBCNews.com who has worked with NBC News Investigations. She reports on health, science and the environment and is a graduate of the Craig Newmark Graduate School of Journalism at City University of New York.
- Skip to main content
- Keyboard shortcuts for audio player
NPR's Book of the Day

- LISTEN & FOLLOW
- Apple Podcasts
- Amazon Music
Your support helps make our show possible and unlocks access to our sponsor-free feed.
'Hurdles in the Dark' is a memoir about a kidnapping, juvenile detention and racing

Elvira K. Gonzalez says there was a lot of beauty to growing up in the culturally rich border town of Laredo, Texas. But there were some challenges, too. Her new memoir, Hurdles in the Dark , chronicles some of the more difficult aspects of her adolescence — her mom was kidnapped, Gonzalez was sent to juvenile detention, and she was preyed upon by her hurdling coaches. In today's episode, the author speaks with Here & Now's Deepa Fernandes about the resilience and optimism she carried through all of that, and how it's gotten her to where she is today.
To listen to Book of the Day sponsor-free and support NPR's book coverage, sign up for Book of the Day+ at plus.npr.org/bookoftheday
To revisit this article, visit My Profile, then View saved stories .

As a Teenager in Europe, I Went to Nudist Beaches All the Time. 30 Years Later, Would the Experience Be the Same?

In July 2017, I wrote an article about toplessness for Vogue Italia. The director, actor, and political activist Lina Esco had emerged from the world of show business to question public nudity laws in the United States with 2014’s Free the Nipple . Her film took on a life of its own and, thanks to the endorsement from the likes of Miley Cyrus, Cara Delevingne, and Willow Smith, eventually developed into a whole political movement, particularly on social media where the hashtag #FreeTheNipple spread at lightning speed. The same year as that piece, actor Alyssa Milano tweeted “me too” and encouraged others who had been sexually assaulted to do the same, building on the movement activist Tarana Burke had created more than a decade earlier. The rest is history.
In that Vogue article, I chatted with designer Alessandro Michele about a shared memory of our favorite topless beaches of our youth. Anywhere in Italy where water appeared—be it the hard-partying Riviera Romagnola, the traditionally chic Amalfi coast and Sorrento peninsula, the vertiginous cliffs and inlets of Italy’s continuation of the French Côte d’Azur or the towering volcanic rocks of Sicily’s mythological Riviera dei Ciclopi—one was bound to find bodies of all shapes and forms, naturally topless.
In the ’90s, growing up in Italy, naked breasts were everywhere and nobody thought anything about it. “When we look at our childhood photos we recognize those imperfect breasts and those bodies, each with their own story. I think of the ‘un-beauty’ of that time and feel it is actually the ultimate beauty,” Michele told me.
Indeed, I felt the same way. My relationship with toplessness was part of a very democratic cultural status quo. If every woman on the beaches of the Mediterranean—from the sexy girls tanning on the shoreline to the grandmothers eating spaghetti al pomodoro out of Tupperware containers under sun umbrellas—bore equally naked body parts, then somehow we were all on the same team. No hierarchies were established. In general, there was very little naked breast censorship. Free nipples appeared on magazine covers at newsstands, whether tabloids or art and fashion magazines. Breasts were so naturally part of the national conversation and aesthetic that Ilona Staller (also known as Cicciolina) and Moana Pozzi, two porn stars, cofounded a political party called the Love Party. I have a clear memory of my neighbor hanging their party’s banner out his window, featuring a topless Cicciolina winking.
A lot has changed since those days, but also since that initial 2017 piece. There’s been a feminist revolution, a transformation of women’s fashion and gender politics, the absurd overturning of Harvey Weinstein’s 2020 rape conviction in New York, the intensely disturbing overturning of Roe v Wade and the current political battle over reproductive rights radiating from America and far beyond. One way or another, the female body is very much the site of political battles as much as it is of style and fashion tastes. And maybe for this reason naked breasts seem to populate runways and street style a lot more than they do beaches—it’s likely that being naked at a dinner party leaves more of a permanent mark than being naked on a glamorous shore. Naked “dressing” seems to be much more popular than naked “being.” It’s no coincidence that this year Saint Laurent, Chloé, Ferragamo, Tom Ford, Gucci, Ludovic de Saint Sernin, and Valentino all paid homage to sheer dressing in their collections, with lacy dresses, see-through tops, sheer silk hosiery fabric, and close-fitting silk dresses. The majority of Anthony Vaccarello’s fall 2024 collection was mostly transparent. And even off the runway, guests at the Saint Laurent show matched the mood. Olivia Wilde appeared in a stunning see-through dark bodysuit, Georgia May Jagger wore a sheer black halter top, Ebony Riley wore a breathtaking V-neck, and Elsa Hosk went for translucent polka dots.
In some strange way, it feels as if the trends of the ’90s have swapped seats with those of today. When, in 1993, a 19-year-old Kate Moss wore her (now iconic) transparent, bronze-hued Liza Bruce lamé slip dress to Elite Model Agency’s Look of the Year Awards in London, I remember seeing her picture everywhere and feeling in awe of her daring and grace. I loved her simple sexy style, with her otherworldly smile, the hair tied back in a bun. That very slip has remained in the collective unconscious for decades, populating thousands of internet pages, but in remembering that night Moss admitted that the nude look was totally unintentional: “I had no idea why everyone was so excited—in the darkness of Corinne [Day’s] Soho flat, the dress was not see-through!” That’s to say that nude dressing was usually mostly casual and not intellectualized in the context of a larger movement.

But today nudity feels loaded in different ways. In April, actor and author Julia Fox appeared in Los Angeles in a flesh-colored bra that featured hairy hyper-realist prints of breasts and nipples, and matching panties with a print of a sewn-up vagina and the words “closed” on it, as a form of feminist performance art. Breasts , an exhibition curated by Carolina Pasti, recently opened as part of the 60th Venice Biennale at Palazzo Franchetti and showcases works that span from painting and sculpture to photography and film, reflecting on themes of motherhood, empowerment, sexuality, body image, and illness. The show features work by Cindy Sherman, Robert Mapplethorpe, Louise Bourgeois, and an incredible painting by Bernardino Del Signoraccio of Madonna dell’Umiltà, circa 1460-1540. “It was fundamental for me to include a Madonna Lactans from a historical perspective. In this intimate representation, the Virgin reveals one breast while nurturing the child, the organic gesture emphasizing the profound bond between mother and child,” Pasti said when we spoke.
Through her portrayal of breasts, she delves into the delicate balance of strength and vulnerability within the female form. I spoke to Pasti about my recent musings on naked breasts, which she shared in a deep way. I asked her whether she too noticed a disparity between nudity on beaches as opposed to the one on streets and runways, and she agreed. Her main concern today is around censorship. To Pasti, social media is still far too rigid around breast exposure and she plans to discuss this issue through a podcast that she will be launching in September, together with other topics such as motherhood, breastfeeding, sexuality, and breast cancer awareness.
With summer at the door, it was my turn to see just how much of the new reread on transparency would apply to beach life. In the last few years, I noticed those beaches Michele and I reminisced about have grown more conservative and, despite being the daughter of unrepentant nudists and having a long track record of militant topless bathing, I myself have felt a bit more shy lately. Perhaps a woman in her 40s with two children is simply less prone to taking her top off, but my memories of youth are populated by visions of bare-chested mothers surveilling the coasts and shouting after their kids in the water. So when did we stop? And why? When did Michele’s era of “un-beauty” end?
In order to get back in touch with my own naked breasts I decided to revisit the nudist beaches of my youth to see what had changed. On a warm day in May, I researched some local topless beaches around Rome and asked a friend to come with me. Two moms, plus our four children, two girls and two boys of the same ages. “Let’s make an experiment of this and see what happens,” I proposed.
The kids all yawned, but my friend was up for it. These days to go topless, especially on urban beaches, you must visit properties that have an unspoken nudist tradition. One of these in Rome is the natural reserve beach at Capocotta, south of Ostia, but I felt a bit unsure revisiting those sands. In my memory, the Roman nudist beaches often equated to encounters with promiscuous strangers behind the dunes. I didn’t want to expose the kids, so, being that I am now a wise adult, I went ahead and picked a compromise. I found a nude-friendly beach on the banks of the Farfa River, in the rolling Sabina hills.
We piled into my friend’s car and drove out. The kids were all whining about the experiment. “We don’t want to see naked mums!” they complained. “Can’t you just lie and say you went to a nudist beach?”
We parked the car and walked across the medieval fairy-tale woods until we reached the path that ran along the river. All around us were huge trees and gigantic leaves. It had rained a lot recently and the vegetation had grown incredibly. We walked past the remains of a Roman road. The colors all around were bright green, the sky almost fluorescent blue. The kids got sidetracked by the presence of frogs. According to the indications, the beach was about a mile up the river. Halfway down the path, we bumped into a couple of young guys in fanny packs. I scanned them for signs of quintessential nudist attitude, but realized I actually had no idea what that was. I asked if we were headed in the right direction to go to “the beach”. They nodded and gave us a sly smile, which I immediately interpreted as a judgment about us as mothers, and more generally about our age, but I was ready to vindicate bare breasts against ageism.
We reached a small pebbled beach, secluded and bordered by a huge trunk that separated it from the path. A group of girls was there, sharing headphones and listening to music. To my dismay they were all wearing the tops and bottoms of their bikinis. One of them was in a full-piece bathing suit and shorts. “See, they are all wearing bathing suits. Please don’t be the weird mums who don’t.”
At this point, it was a matter of principle. My friend and I decided to take our bathing suits off completely, if only for a moment, and jumped into the river. The boys stayed on the beach with full clothes and shoes on, horrified. The girls went in behind us with their bathing suits. “Are you happy now? my son asked. “Did you prove your point?”
I didn’t really know what my point actually was. I think a part of me wanted to feel entitled to those long-gone decades of naturalism. Whether this was an instinct, or as Pasti said, “an act that was simply tied to the individual freedom of each woman”, it was hard to tell. At this point in history, the two things didn’t seem to cancel each other out—in fact, the opposite. Taking off a bathing suit, at least for my generation who never had to fight for it, had unexpectedly turned into a radical move and maybe I wanted to be part of the new discourse. Also, the chances of me going out in a fully sheer top were slim these days, but on the beach it was different. I would always fight for an authentic topless experience.
After our picnic on the river, we left determined to make our way—and without children—to the beaches of Capocotta. In truth, no part of me actually felt very subversive doing something I had been doing my whole life, but it still felt good. Once a free breast, always a free breast.
This article was originally published on British Vogue .
More Great Living Stories From Vogue
Meghan Markle Is Returning to Television
Is Art Deco Interior Design Roaring Back Into Style?
Kate Middleton and Prince William Share a Never-Before-Seen Wedding Picture
Sofia Richie Grainge Has Given Birth to Her First Child—And the Name Is…
The 10 Best Spas in the World
Never miss a Vogue moment and get unlimited digital access for just $2 $1 per month.
Vogue Daily
By signing up you agree to our User Agreement (including the class action waiver and arbitration provisions ), our Privacy Policy & Cookie Statement and to receive marketing and account-related emails from Vogue. You can unsubscribe at any time. This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
International Spillovers of U.S. Fiscal Challenges
Expansionary fiscal policies have increased significantly following the subprime crisis in 2007 and the COVID-19 crisis, leading to fiscal dominance concerns, where a growing share of monetary authorities may be forced to deviate from policy targets to accommodate fiscal policies. Meanwhile, peripheral economies are constantly influenced by monetary and fiscal conditions in center economies, with the United States (U.S.) as the predominant force. In light of these developments, we examine the potential international spillovers from U.S. inflationary spells and growing fiscal concerns to the policy interest rates in Emerging Market Economies (EMEs) and Developed Economies (DEs). We introduce a new index of fiscal dominance concerns using Principal Components Analysis, and extend the concept to an international perspective, as opposed to previous literature examining fiscal dominance in a domestic environment. The results are confirmed by robustness analysis and show that greater U.S. fiscal challenges affect negatively the policy rates in both EMEs and DEs, with a greater impact observed in EMEs. Moreover, a low degree of financial repression is associated with more significant spillover effects from greater U.S. fiscal challenges.
An earlier version of this paper was presented at the economics division of Linköping University, Sweden. The authors are deeply grateful to Bo Sjö, Donghyun Park, Jamel S., Ayhan Kose, Franziska Ohnsorge, and Naotaka Sugawara for sharing the fiscal space data. Joshua Aizenman gratefully acknowledges the financial support of the Dockson Chair at the University of Southern California The views expressed herein are those of the authors and do not necessarily reflect the views of the National Bureau of Economic Research and the Asian Development Bank.
MARC RIS BibTeΧ
Download Citation Data
More from NBER
In addition to working papers , the NBER disseminates affiliates’ latest findings through a range of free periodicals — the NBER Reporter , the NBER Digest , the Bulletin on Retirement and Disability , the Bulletin on Health , and the Bulletin on Entrepreneurship — as well as online conference reports , video lectures , and interviews .

Essay Service Examples Psychology Adolescence
Understanding Adolescence Essay: Challenges and Solutions in the USA
Table of contents
What is adolescence, problems of adolescence, how can these problems be solved.
- Proper editing and formatting
- Free revision, title page, and bibliography
- Flexible prices and money-back guarantee

Our writers will provide you with an essay sample written from scratch: any topic, any deadline, any instructions.
Cite this paper
Related essay topics.
Get your paper done in as fast as 3 hours, 24/7.
Related articles

Most popular essays
- Adolescence
Every 40 seconds an individual commits suicide, making it the tenth leading cause of death...
- Self Esteem
There are two critical aspects of personality that can determine a person’s self worth - self...
Lito is an eighteen-year-old male. He claims he plays electronic sports for four to five hours a...
Rena has a height of 5’5” while Ashley has a height of 5’6”. They are 17 years old and on their 12...
Sleep is vital for the human body to function but due to the stressful and busy life of...
Did you know that archery is the second oldest sport in the world? This fact proves that sport...
- Juvenile Delinquency
Juvenile Delinquency has been an ongoing phenomenon for years and will unfortunately continue in...
This criminal justice research paper is an analysis of the family dynamics affecting juvenile...
Body image dissatisfaction continues to be a major concern in America’s youth, especially in...
Join our 150k of happy users
- Get original paper written according to your instructions
- Save time for what matters most
Fair Use Policy
EduBirdie considers academic integrity to be the essential part of the learning process and does not support any violation of the academic standards. Should you have any questions regarding our Fair Use Policy or become aware of any violations, please do not hesitate to contact us via [email protected].
We are here 24/7 to write your paper in as fast as 3 hours.
Provide your email, and we'll send you this sample!
By providing your email, you agree to our Terms & Conditions and Privacy Policy .
Say goodbye to copy-pasting!
Get custom-crafted papers for you.
Enter your email, and we'll promptly send you the full essay. No need to copy piece by piece. It's in your inbox!
Please log in to save materials. Log in
- Adolescent Psychology
Challenges of Adolescence

Recognizing adolescence
Adolescence is a period of life with specific health and developmental needs and rights. It is also a time to develop knowledge and skills, learn to manage emotions and relationships, and acquire attributes and abilities that will be important for enjoying the adolescent years and assuming adult roles.
All societies recognize that there is a difference between being a child and becoming an adult. How this transition from childhood to adulthood is defined and recognized differs between cultures and over time. In the past it has often been relatively rapid, and in some societies it still is. In many countries, however, this is changing.
Age: not the whole story
Age is a convenient way to define adolescence. But it is only one characteristic that delineates this period of development. Age is often more appropriate for assessing and comparing biological changes (e.g. puberty), which are fairly universal, than the social transitions, which vary more with the socio-cultural environment.
CHALLENGES OF ADOLESCENCE
Adolescence is a time in a young person’s life where they move from dependency on their parents to independence, autonomy and maturity. The young person begins to move from the family group being their major social system, to the family taking a lesser role and being part of a peer group becomes a greater attraction that will eventually lead to the young person to standing alone as an adult.
No-one can deny that for any one person facing changes in their lives in the biological, cognitive, psychological, social, moral and spiritual sense, could find this time both exciting and daunting. With the increase in independence comes increases in freedom, but with that freedom, comes responsibilities. Attitudes and perspectives change and close family members often feel they are suddenly living with a stranger.
Biological Challenges
Adolescence begins with the first well-defined maturation event called puberty. Included in the biological challenges are the changes that occur due to the release of the sexual hormones that affect emotions. Mood changes can increase, which can impact on relationships both at home with parents and siblings and socially or at school.
Cognitive Challenges
Piaget, in his theory of social development believed that adolescence is the time when young people develop cognitively from “concrete operations” to “formal operations”. So they are able to deal with ideas, concepts and abstract theories. It takes time for confidence to build with using these newly acquired skills, and they may make mistakes in judgement. Learning through success and failure is part of the challenge of the learning process for the adolescent.
Adolescents are egocentric, they can become self-conscious; thinking they are being watched by others, and at other times want to behave as if they were on a centre stage and perform for a non-existent audience. For example, acting like a music idol, singing their favourites songs in their room, with all the accompanying dance steps.
Psychological Challenges
The psychological challenges that the adolescent must cope with are moving from childhood to adulthood. A new person is emerging, where rules will change, maybe more responsibilities will be placed on him/her so that a certain standard of behaviour is now required to be maintained. Accountability is becoming an expectation from both a parental and legal concept.
As adolescents continue their journey of self-discovery, they continually have to adjust to new experiences as well as the other changes happening to them biologically and socially. This can be both stressful and anxiety provoking. It therefore is not surprising that adolescents can have a decreased tolerance for change; hence it becomes increasingly more difficult for them to modulate their behaviours which are sometimes displayed by inappropriate mood swings and angry outbursts.
Health Issues of adolescence:
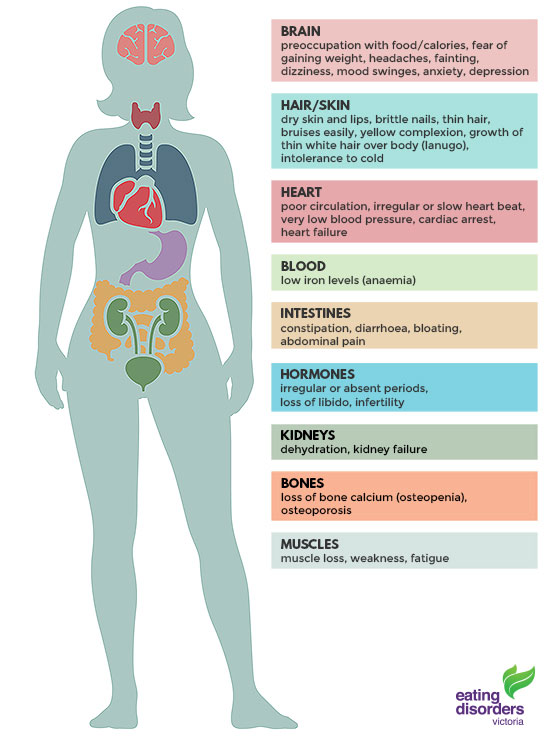
Eating Disorders
An eating disorder is a serious mental illness, characterised by eating, exercise and body weight or shape becoming an unhealthy preoccupation of someone's life. Eating disorders are not a lifestyle choice, a diet gone wrong or a cry for attention. Eating disorders can take many different forms and interfere with a person’s day to day life.
Types of Eating Disorders
An eating disorder is commonly defined as an all-consuming desire to be thin and/or an intense fear of weight gain. The most common eating disorders among adolescents are anorexia, bulimia and binge-eating disorder. Even patients that do not meet all of the clinical criteria for an eating disorder can be at serious risk and should seek medical treatment.
Anorexia Nervosa
Teenagers with anorexia may take extreme measures to avoid eating and control the quantity and quality of the foods they do eat. They may become abnormally thin, or thin for their body, and still talk about feeling fat. They typically continue to diet even at very unhealthy weights because they have a distorted image of their body.
Signs of anorexia nervosa
- A distorted view of one’s body weight, size or shape; sees self as too fat, even when very underweight
- Hiding or discarding food
- Obsessively counting calories and/or grams of fat in the diet
- Denial of feelings of hunger
- Developing rituals around preparing food and eating
- Compulsive or excessive exercise
- Social withdrawal
- Pronounced emotional changes, such as irritability, depression and anxiety
Physical signs of anorexia include rapid or excessive weight loss; feeling cold, tired and weak; thinning hair; absence of menstrual cycles in females; and dizziness or fainting.
Teenagers with anorexia often restrict not only food, but relationships, social activities and pleasurable experiences.
Physical Signs and Effects of Anorexia Nervosa
Bulimia Nervosa
Teenagers with bulimia nervosa typically ‘binge and purge’ by engaging in uncontrollable episodes of overeating (bingeing) usually followed by compensatory behavior such as: purging through vomiting, use of laxatives, enemas, fasting, or excessive exercise. Eating binges may occur as often as several times a day but are most common in the evening and night hours.
Teenagers with bulimia often go unnoticed due to the ability to maintain a normal body weight.
Bulimia Nervosa often starts with weight-loss dieting. The resulting food deprivation and inadequate nutrition can trigger what is, in effect, a starvation reaction - an overriding urge to eat. Once the person gives in to this urge, the desire to eat is uncontrollable, leading to a substantial binge on whatever food is available (often foods with high fat and sugar content), followed by compensatory behaviours. A repeat of weight-loss dieting often follows, leading to a binge/purge/exercise cycle which becomes more compulsive and uncontrollable over time.
Signs of bulimia nervosa
- Eating unusually large amounts of food with no apparent change in weight
- Hiding food or discarded food containers and wrappers
- Excessive exercise or fasting
- Peculiar eating habits or rituals
- Frequent tips to the bathroom after meals
- Inappropriate use of laxatives, diuretics, or other cathartics
- Overachieving and impulsive behaviors
- Frequently clogged showers or toilets
Physical signs of bulimia include discolored teeth, odor on the breath, stomach pain, calluses/scarring on the hands caused by self-inducing vomiting, irregular or absent menstrual periods, and weakness or fatigue.
Teenagers with bulimia often have a preoccupation with body weight and shape, as well as a distorted body image. The clinical diagnosis commonly defines a teenager as having bulimia if they binge and purge on average once a week for at least three consecutive months.
Physical Signs and Effects of Bulimia Nervosa
Sexually Transmitted Diseases
Sexually transmitted diseases (STDs) are infections that are passed from one person to another through sexual contact. The causes of STDs are bacteria, parasites, yeast, and viruses. There are more than 20 types of STDs, including
Genital herpes
- Trichomoniasis
Most STDs affect both men and women, but in many cases the health problems they cause can be more severe for women. If a pregnant woman has an STD, it can cause serious health problems for the baby.
Antibiotics can treat STDs caused by bacteria, yeast, or parasites. There is no cure for STDs caused by a virus, but medicines can often help with the symptoms and keep the disease under control.
Correct usage of latex condoms greatly reduces, but does not completely eliminate, the risk of catching or spreading STDs. The most reliable way to avoid infection is to not have anal, vaginal, or oral sex.
Chlamydia is an STD caused by Chlamydia trachomatis (C. trachomatis). This bacterium only infects humans. Chlamydia is the most common infectious cause of genital and eye diseases globally. It is also the most common bacterial STD.
Women with chlamydia do not usually show symptoms. Any symptoms are usually non-specific and may include:
- bladder infection
- a change in vaginal discharge
- mild lower abdominal pain
If a person does not receive treatment for chlamydia, it may lead to the following symptoms:
- pelvic pain
- painful sexual intercourse, either intermittently or every time
- bleeding between periods
This STD is caused by the herpes simplex virus (HSV). The virus affects the skin, cervix, genitals, and some other parts of the body. There are two types:
- HSV-1, also known as herpes type 1
- HSV-2, also known as herpes type 2
Herpes is a chronic condition. A significant number of individuals with herpes never show symptoms and do not know about their herpes status.
HSV is easily transmissible from human to human through direct contact. Most commonly, transmission of type 2 HSV occurs through vaginal, oral, or anal sex. Type 1 is more commonly transmitted from shared straws, utensils, and surfaces.
In most cases, the virus remains dormant after entering the human body and shows no symptoms.
Symptoms of genital herpes
- blisters and ulceration on the cervix
- vaginal discharge
- pain on urinating
- generally feeling unwell
- cold sores around the mouth in type 1 HSV
This sexually transmitted bacterial infection usually attacks the mucous membranes. It is also known as the clap or the drip. The bacterium, which is highly contagious, stays in the warmer and moister cavities of the body.
The majority of women with gonorrhea show no signs or symptoms. If left untreated, females may develop pelvic inflammatory disease (PID). Males may develop inflammation of the prostate gland, urethra, or epididymis.
The disease is caused by Neisseria gonorrhoeae. The bacteria can survive in the vagina, penis, mouth, rectum, or eye. They can be transmitted during sexual contact.
Symptoms of gonorrhea may occur between 2 to 10 days after initial infection, in some cases, it may take 30 days. Some people experience very mild symptoms that lead to mistaking gonorrhea for a different condition, such as a yeast infection.
Males may experience the following symptoms:
- burning during urination
- testicular pain or swelling
- a green, white, or yellow discharge from the penis
Females are less likely to show symptoms, but if they do, these may include:
- spotting after sexual intercourse
- swelling of the vulva, or vulvitis
- irregular bleeding between periods
- pink eye, or conjunctivitis
- pain in the pelvic area
- burning or pain during urination
HIV and AIDS
Human immunodeficiency virus (HIV) attacks the immune system, leaving its host much more vulnerable to infections and diseases. If the virus is left untreated, the susceptibility to infection worsens.
HIV can be found in semen, blood, breast milk, and vaginal and rectal fluids. HIV can be transmitted through blood-to-blood contact, sexual contact, breast-feeding, childbirth, the sharing of equipment to inject drugs, such as needles and syringes, and, in rare instances, blood transfusions.
With treatment, the amount of the virus present within the body can be reduced to an undetectable level. This means the amount of HIV virus within the blood is at such low levels that it cannot be detected in blood tests. It also means that HIV cannot be transmitted to other people. A person with undetectable HIV must continue to take their treatment as normal, as the virus is being managed, not cured.
HIV is a virus that targets and alters the immune system, increasing the risk and impact of other infections and diseases. Without treatment, the infection might progress to an advanced disease stage 3 called AIDS. However, modern advances in treatment mean that people living with HIV in countries with good access to healthcare very rarely develop AIDS once they are receiving treatment.
Mental Health Disorder
1.Anxiety Disorders
Anxiety disorders are a group of mental disorders characterized by significant feelings of anxiety and fear. Anxiety is a worry about future events, and fear is a reaction to current events. These feelings may cause physical symptoms, such as a fast heart rate and shakiness.
Occasional anxiety is an expected part of life. You might feel anxious when faced with a problem at work, before taking a test, or before making an important decision. But anxiety disorders involve more than temporary worry or fear. For a person with an anxiety disorder, the anxiety does not go away and can get worse over time. The symptoms can interfere with daily activities such as job performance, school work, and relationships.
There are several types of anxiety disorders, including generalized anxiety disorder, panic disorder, and various phobia-related disorders.
Generalized Anxiety Disorder
People with generalized anxiety disorder (GAD) display feel excessive, unrealistic worry and tension with little or no reason , most days for atleast 6 months, about a number of things such as personal health, work, social interactions, and everyday routine life circumstances. The fear and anxiety can cause significant problems in areas of their life, such as social interactions, school, and work.
Generalized anxiety disorder symptoms include:
- Feeling restless, wound-up, or on-edge
- Being easily fatigued
- Having difficulty concentrating; mind going blank
- Being irritable
- Having muscle tension
- Difficulty controlling feelings of worry
- Having sleep problems, such as difficulty falling or staying asleep, restlessness, or unsatisfying sleep
Panic Disorder
People with panic disorder have recurrent unexpected panic attacks. Panic attacks are sudden periods of intense fear that come on quickly and reach their peak within minutes. Attacks can occur unexpectedly or can be brought on by a trigger, such as a feared object or situation.
During a panic attack, people may experience:
- Heart palpitations ( unusually strong or irregular heartbeats) , a pounding heartbeat, or an accelerated heart rate.
- Trembling or shaking
- Sensations of shortness of breath, smothering, or choking
- Feelings of impending doom
- Feelings of being out of control
People with panic disorder often worry about when the next attack will happen and actively try to prevent future attacks by avoiding places, situations, or behaviors they associate with panic attacks. Worry about panic attacks, and the effort spent trying to avoid attacks, because significant problems in various areas of the person’s life, including the development of agoraphobia - People with agoraphobia have an intense fear of two or more of the following situations:
- Using public transportation
- Being in open spaces
- Being in enclosed spaces
- Standing in line or being in a crowd
- Being outside of the home alone
2. Mood Disorders
The development of emotional or behavioral symptoms in response to an identifiable stressors that occur within 3 months of the onset of the stressors in which low mood, tearfulness, or feelings of hopelessness are predominant.
3. Major Depressive Disorder (MDD):
A period of atleast 2 weeks during which there is either depressed mood or the loss of interest or pleasure in nearly all activities. In children and adolescents, the mood may be irritable rather than sad.
4. Bipolar Disorder:
A period of abnormally and persistently elevated, expansive, or irritable mood and abnormally and persistency increased activity or energy, lasting at least 4 consecutive days and present most of the day, nearly every day, or that requires hospitalization.
5. Attention Deficit Hyperactivity Disorder
Definitions of the symptom complex known as attention-deficit/hyperactivity disorder (ADHD) differ, but severe problems with concentration or attention and/or hyperactivity are estimated to affect adolescents. Six times as many boys as girls are affected. The main consequences of ADHD are poor academic performance and behavioural problems, although adolescents with ADHD are at substantially higher risk of serious accidents, depression, and other psychological problems. About 80% of children with ADHD continue to have the disorder during adolescence, and as many as 50% of adolescents still do throughout adulthood.
6. School phobia
School phobia also called school refusal, is defined as a persistent and irrational fear of going to school. It must be distinguished from a mere dislike of school that is related to issues such as a new teacher, a difficult examination, the class bully, lack of confidence, or having to undress for a gym class. The phobic adolescent shows an irrational fear of school and may show marked anxiety symptoms when in or near the school.
7. Learning disabilities
Learning abilities encompasses disorders that affect the way individuals with normal or above normal intelligence receive, store, organize, retrieve, and use information. Problems included dyslexia and other specific learning problems involving reading, spelling, writing, reasoning, and mathematics. Undiagnosed learning disabilities are a common but managerable cause of young people deciding to leave school at the earliest opportunity.
Social Issues
Sexual Abuse
Sexual abuse is sexual behavior or a sexual act forced upon a woman, man or child without their consent. Sexual abuse includes abuse of a woman, man or child by a man, woman or child.
Sexual abuse or violence against children and adolescents is defined as a situation in which children or adolescents are used for the sexual pleasure of an adult or older adolescent, (legally responsible for them or who has some family relationship, either current or previous), which ranges from petting, fondling of genitalia, breasts or anus, sexual exploitation, voyeurism, pornography, exhibitionism, to the sexual intercourse itself, with or without penetration.
Sexual abuse in childhood may result in problems of depression and low self-esteem as well as in sexual difficulties, either avoidance of sexual contact or, on the other hand, promiscuity or prostitution. Research studies suggest that the kinds of abuse that appear to be the most damaging are those that involve father figures, genital contact, and force.
As reports of sexual abuse of children have increased, ways to protect children are now being carried out. Some information campaigns have concentrated on children’s contacts with strangers-for example, “Never get into a car with anyone you don’t know, “Never go with someone who says he or she has some candy for you”. However, in the majority of reported assaults children are victimized by people they know. To prevent this kind of assaults, children need to be taught to recognize signs of trouble and to be assertive enough to report them to a responsible adult. How to accomplish this task represents an important challenge to prevention-oriented researchers.
Sexual abuse of children is regarded by the World Health Organization (WHO) as one of the major public health problems. Studies conducted in different countries suggest that 7-36% of girls and 3-29% of boys suffered sexual abuse.
Substance Abuse
Many communities are plagued with problems of substance abuse among youth. Some children start smoking or chewing tobacco at an early age, aided by easy access to tobacco products. Many of our youth, with limited supervision or few positive alternatives, drink too much beer and liquor. Other youth, influenced by their peers, use other illegal drugs. Our youth suffer from substance abuse in familiar ways: diminished health, compromised school performance, and reduced opportunities for development. Our communities also bear a heavy burden for adolescent substance abuse. Widespread use and abuse of tobacco, alcohol, and illegal drugs by teens can result in increased accidents, health costs, violence, crime, and an erosion of their future potential as workers and citizens.
Protective factors are personal and environmental factors that decrease the likelihood that a person may experience a particular problem. Protective factors act as buffers against risk factors and are frequently the inverse of risk factors.
Personal risk factors for substance abuse include: poor school grades, low expectations for education, school dropout, poor parent communication, low self-esteem, strong negative peer influences, peer use, lack of perceived life options, low religiosity, lack of belief about risk, and involvement in other high-risk behaviours. Environmental risk factors include: lack of parental support, parental practice of high-risk behaviors, lack of resources in the home, living in an urban area, poor school quality, availability of substances, community norms favorable to substance use, extreme economic deprivation, and family conflict.
Protective factors may include peer tutoring to improve school grades, mentoring and scholarship programs to increase educational opportunities, programs to build strong communication and refusal Preface Work Group for Community Health and Development iv skills, information to increase understanding about risk, and the enforcement of local laws prohibiting the illegal sale of tobacco and alcohol products to youth.
Influence of Electronic Media
Electronic devices are an integral part of adolescent's lives in the twenty-first century. The world of electronic devices, however, is changing dramatically. Television, which dominated the media world through the mid-1990s, now competes in an arena crowded with cell phones, computers, iPods, video games, instant messaging, interactive multiplayer video games, virtual reality sites, Web social networks, and e-mail.
Electronic devices are defined as any object or process of human origin that can be used to convey media as books, films, mobiles, television, and the Internet. With respect to education, communication or play.
Adolescents, in particular, spend a significant amount of time in viewing and interacting with electronic devices in the form of TV, video games, music, and the Internet. Considering all of these sources together, adolescence spend more than six hours per day using media. Nearly half of that time is spent in watching TV, playing, or studying with computer. The remainder of the time is spent using other electronic media alone or in combination with TV.
The electronic media mainly consist of radio, television, and movies, and are actually classrooms without four walls. Media is an important source of shared images and messages relating to political and social context. Technology of media is an important part of student’s lives in the twenty-first century and play very important role in creating awareness related various aspects of life and personality as found. The world of electronic media, however, is changing dramatically. Television, which dominated the media world through the mid-1990s, now competes with cell phones, iPods, video games, instant messaging, interactive multiplayer video games, Web social networks, and e-mail. We learn skills, values and patterns of behavior from the media both directly and indirectly. There is no doubt that electronic media have a important influence on children from a very early age, and that it will continue to affect children's cognitive and social development. Electronic media activate and reinforce attitude and contribute significantly in the formation of new attitudes.
Effects of Technology on Adolescence
Technology and internet addiction in adolescence can have far reaching effects on the addict and his family. Adolescence with technology addiction can suffer from a variety of physical and psychological health problems.
General Effects
- Poor eating habits
- Increased obesity
- Attention problems in school, low attention span
- Lack of empathy
- Poor academic performance
- Social phobia
- Increased instances of cyberbullying
- Increased instances of substance abuse
- Growth issues
- Unable to control impulse to use the Internet/technology
- Feelings of happiness when using Internet or thinking about using the Internet
Negative effects of video games on adolescence's physical health, including obesity, video-induced seizures and postural, muscular and skeletal disorders, such as tendonitis, nerve compression, and carpal tunnel syndrome as well as delayed school achievement. However, these effects are not likely to occur for most adolescence. Parents should be most concerned about two things: the amount of time that adolescence play, and the content of the what to be play or watching.
In addition, symptoms associated with using mobile phones most commonly include headaches, earache, warmth sensations and sometimes also perceived concentration difficulties as well as fatigue However, over exposure to mobile phone use is not currently known to have major health effects. Another aspect of exposure is ergonomics. Musculoskeletal symptoms due to intensive texting on a mobile phone have been reported and techniques used for text entering have been studied in connection with developing musculoskeletal symptoms. The central factors appearing to explain high quantitative use were personal dependency, and demands for achievement and availability originating from domains of work,
To protect adolescence from harm, all health staff must have the competences to recognize adolescence maltreatment and to take effective action as appropriate to their role. They must also clearly understand their responsibilities, and should be supported by their employing organization. In addition, Parents have no idea about electronic devices effects on adolescence. So, parents need to understand that electronic devices can have an impact on everything they are concerned about with their adolescence's health and development, school performance, learning disabilities, sex, drugs, and aggressive behavior.
Preventive Measures
- Set strict time limit for phone use at home.
- Restrict the use of video games, television and other gadgets.
- Ask your teens to use only the family computer for all their online activities at home.
- Supervise the time your teens spend on the Internet.
- Spend time with your child to understand the source of his addiction. It is important for parents to know what makes their children find solace on the Internet.
- Talk to your teen’s teachers to understand problems at school, if any.
- Create positive environment at home. Your teen could be spending excessive time on the Internet to escape the problems at home. This excessive time spend on technology can easily turn into an addiction.
- Enforce no-Internet time at home or consequences for breaking rules about using technology at home.
Version History
Numbers, Facts and Trends Shaping Your World
Read our research on:
Full Topic List
Regions & Countries
- Publications
- Our Methods
- Short Reads
- Tools & Resources
Read Our Research On:
The concerns and challenges of being a U.S. teen: What the data show

American teens have a lot on their minds. Substantial shares point to anxiety and depression, bullying, and drug and alcohol use (and abuse) as major problems among people their age, according to a new Pew Research Center survey of youth ages 13 to 17.
How common are these and other experiences among U.S. teens? We reviewed the most recent available data from government and academic researchers to find out:
Anxiety and depression
Serious mental stress is a fact of life for many American teens. In the new survey, seven-in-ten teens say anxiety and depression are major problems among their peers – a concern that’s shared by mental health researchers and clinicians .

Data on the prevalence of anxiety disorders is hard to come by among teens specifically. But 7% of youths ages 3 to 17 had such a condition in 2016-17, according to the National Survey of Children’s Health. Serious depression, meanwhile, has been on the rise among teens for the past several years, according to the National Survey on Drug Use and Health , an ongoing project of the federal Department of Health and Human Services. In 2016, 12.8% of youths ages 12 to 17 had experienced a major depressive episode in the past year, up from 8% as recently as 2010. For 9% of youths in 2016, their depression caused severe impairment. Fewer than half of youths with major depression said they’d been treated for it in the past year.
Alcohol and drugs
Anxiety and depression aren’t the only concerns for U.S. teens. Smaller though still substantial shares of teens in the Pew Research Center survey say drug addiction (51%) and alcohol consumption (45%) are major problems among their peers.

Fewer teens these days are drinking alcohol, according to the University of Michigan’s long-running Monitoring the Future survey, which tracks attitudes, values and behaviors of American youths, including their use of various legal and illicit substances. Last year, 30.2% of 12th-graders and 18.6% of 10th-graders had consumed alcohol in the past 30 days. Two decades earlier, those figures were 52% and 38.8%, respectively. (In the Center’s new survey, 16% of teens said they felt “a lot” or “some” pressure to drink alcohol.)
But the Michigan survey also found that, despite some ups and downs, use of marijuana (or its derivative, hashish) among 12th-graders is nearly as high as it was two decades ago. Last year, 22.2% reported using marijuana in the past 30 days, versus 22.8% in 1998. Past-month marijuana use among 10th-graders has declined a bit over that same period, from 18.7% to 16.7%, but is up from 14% in 2016.
Marijuana was by far the most commonly used drug among teens last year, as it has been for decades. While more than 10% of 12th-graders reported using some illicit drug other than marijuana in the late 1990s and early 2000s, that figure had fallen to 6% by last year.
The Michigan researchers noted that vaping, of both nicotine and marijuana, has jumped in popularity in the past few years. In 2018, 20.9% of 12th-graders and 16.1% of 10th-graders reported vaping nicotine in the past 30 days, about double the 2017 levels. By comparison, only 7.6% of 12th-graders and 4.2% of 10th-graders had smoked a cigarette in that time. And 7.5% of 12-graders and 7% of 10th-graders said they’d vaped marijuana within the past month, up from 4.9% and 4.3%, respectively, in 2017.
Bullying and cyberbullying
Issues of personal safety also are on U.S. teens’ minds. The Center’s survey found that 55% of teens said bullying was a major problem among their peers, while a third called gangs a major problem.

Bullying rates have held steady in recent years, according to a survey of youth risk behaviors by the Centers for Disease Control and Prevention. About a fifth of high school students (19% in 2017) reported being bullied on school property in the past 12 months, and 14.9% said they’d experienced cyberbullying (via texts, social media or other digital means) in the previous year. In both cases, girls, younger students, and students who identified as gay, lesbian or bisexual were more likely to say they’d been bullied.
As for gangs, the share of students ages 12 to 18 who said gangs were present at their school fell from 20.1% in 2001 to 10.7% in 2015, according to a report on school safety from the federal departments of Education and Justice. Black and Hispanic students, as well as students in urban schools, were most likely to report the presence of gangs at school, but even for those groups the shares reporting this fell sharply between 2001 and 2015, the most recent year for which data are available.
Four-in-ten teens say poverty is a major problem among their peers, according to the Center’s new report. In 2017, about 2.2 million 15- to 17-year-olds (17.6%) were living in households with incomes below the poverty level – up from 16.3% in 2009, but down from 18.9% in 2014, based on our analysis of Census data. Black teens were more than twice as likely as white teens to live in households below the poverty level (30.4% versus 14%); however, the share of white teens in below-poverty-level households had risen from 2009 (when it was 12.1%), while the share of black teens in below-poverty-level households was almost unchanged.
Teen pregnancy
Far fewer U.S. teens are having to juggle adolescence and parenthood, as teen births continue their long-term decline . Among 15- to 19-year-olds, the overall birthrate has fallen by two-thirds since 1991 – from 61.8 live births per 1,000 women to 20.3 in 2016 , according to the CDC. All racial and ethnic groups have witnessed teen-birthrate declines of varying degrees: Among non-Hispanic blacks, for example, the rate fell from 118.2 live births per 1,000 in 1991 to 29.3 in 2016 .
- Age & Generations
- Drug Policy
- Health Policy
- Medicine & Health
- Teens & Youth

Drew DeSilver is a senior writer at Pew Research Center .
U.S. adults under 30 have different foreign policy priorities than older adults
Across asia, respect for elders is seen as necessary to be ‘truly’ buddhist, teens and video games today, as biden and trump seek reelection, who are the oldest – and youngest – current world leaders, how teens and parents approach screen time, most popular.
901 E St. NW, Suite 300 Washington, DC 20004 USA (+1) 202-419-4300 | Main (+1) 202-857-8562 | Fax (+1) 202-419-4372 | Media Inquiries
Research Topics
- Email Newsletters
ABOUT PEW RESEARCH CENTER Pew Research Center is a nonpartisan fact tank that informs the public about the issues, attitudes and trends shaping the world. It conducts public opinion polling, demographic research, media content analysis and other empirical social science research. Pew Research Center does not take policy positions. It is a subsidiary of The Pew Charitable Trusts .
© 2024 Pew Research Center
- Entertainment
- Environment
- Information Science and Technology
- Social Issues
Home Essay Samples Psychology Adolescence
My Adolescent Experience and Development: A Reflection

Table of contents
Adolescent experience in my life, physical development, emotional development.
“Perhaps you looked in the mirror on a daily, or sometimes even hourly, basis as a young teenager to see whether you could detect anything different about your changing body. Preoccupation with one’s body image is strong through adolescence, it is especially acute during puberty, a time when adolescents are more dissatisfied with their bodies than in late adolescence.” (Santrock)
Social changes
- Arnett, J. J. (2015). Adolescence and emerging adulthood : A cultural approach. Pearson Education.
- Erikson, E. H. (1968). Identity: Youth and crisis. WW Norton & Company.
- Gullotta, T. P., & Adams, G. R. (Eds.). (2016). Handbook of adolescent behavioral problems: Evidence-based approaches to prevention and treatment. Springer.
- Steinberg, L. (2014). Age of opportunity: Lessons from the new science of adolescence. Houghton Mifflin Harcourt.
- Steinberg, L., & Morris, A. S. (2001). Adolescent development. Annual review of psychology, 52(1), 83-110.
- Suler, J. R. (2018). Adolescent development. In Psychology of Adolescence (pp. 11-38). Springer.
- Rutter, M., & Smith, DJ (1995). Psychosocial disorders in young people: Time trends and their causes. John Wiley & Sons.
- American Psychological Association. (2019). APA handbook of the psychology of adolescence.
- Offer, D., & Schonert-Reichl, K. A. (1992). Debunking the myths of adolescence: Findings from recent research. Journal of the American Academy of Child & Adolescent Psychiatry, 31(6), 1003-1014.
*minimum deadline
Cite this Essay
To export a reference to this article please select a referencing style below

- Confirmation Bias
- Operant Conditioning
- Jean Piaget
- Psychoanalysis
- Reward System
Related Essays
Need writing help?
You can always rely on us no matter what type of paper you need
*No hidden charges
100% Unique Essays
Absolutely Confidential
Money Back Guarantee
By clicking “Send Essay”, you agree to our Terms of service and Privacy statement. We will occasionally send you account related emails
You can also get a UNIQUE essay on this or any other topic
Thank you! We’ll contact you as soon as possible.
Psychology Discussion
Essay on adolescence: top 5 essays | psychology.
ADVERTISEMENTS:
Here is a compilation of essays on ‘Adolescence’ for class 11 and 12. Find paragraphs, long and short essays on ‘Adolescence’ especially written for school and college students.
Essay on Adolescence
Essay Contents:
- Essay on the Meaning of Adolescence
- Essay on the Historical Perspectives of Adolescence
- Essay on the Developmental Model in Adolescence
- Essay on the Factors Influencing Development During Adolescence
- Essay on Developmental Psychopathology during the Period of Adolescence
Essay # 1. Meaning of Adolescence :
Adolescence is a time of rapid physiological and psychological change of intensive readjustment to the family, school, work and social life and of preparation for adult roles.
It starts with puberty and ends with the achievement of an adult work role. It usually begins between 11 and 16 years in boys and between 9 and 16 years in girls. Websters’ dictionary (1977) defines adolescence the ‘process of growing up’ or the ‘period of life from puberty to maturity’. Adolescence has been associated with an age span, varying from 10-13 as the starting age and 19-21 as the concluding age, depending on whose definition is being applied.
Essay # 2. Historical Perspectives of Adolescence :
The concept of adolescence was formally inducted in psychology from 1880. The definitive description of adolescence was given in the two volume work of Stanley Hall in 1904. Hall described adolescence as a period both of upheaval, suffering, passion and rebellion against adult authority and of physical, intellectual and social change.
Anna Freud, Mohr and Despres and Bios have independently affirmed adolescent regression, psychological upheaval, and turbulence as intrinsic to normal adolescence development. Margaret Mead believed adolescence as a ‘cultural invention’.
Albert Bandura said that children and adolescents imitate the behaviour of others especially influential adults ‘entertainment’ heroes and peers. Erikson elaborated the classic psychoanalytic views shifting the emphasis from biological imperatives of the entry into adolescence to focus on psychological challenges in making the transition from adolescence to adulthood (developmental model discussed below).
Piaget proposed a theory of cognitive development describing four major stages in intellectual development. Puberty is a universal process involving dramatic changes in size, shape and appearance. Tanner has described bodily changes of puberty into five stages. The enumeration of Tanner stages is given in Table 28.1.
The relationships between pubertal maturation and psychological development can be considered in two broad models,
(a) The ‘Direct Effect Model’ in which certain psychological effects are directly result of physiological sources,
(b) ‘Mediated Effects Model’ which proposes that the psychological effects of puberty are mediated by complex relations of intervening variables (such as the level of ego development) or are moderated by contexual factors (such as the socio-cultural and socialization practices). In recent days, this model is more favoured.
Essay # 3. Developmental Model in Adolescence :
Developmental theories of adolescence are:
(a) Cognitive development:
Jean Piaget described four distinct stages in the cognitive development from birth to adolescence.
(i) Sensory-motor stage:
Sensory-motor stage (from birth to 18 months) wherein the child acquires numerous basic skills with limited intellectual capacity and is primitive.
(ii) Preoperational or intuitive stage:
Preoperational or intuitive stage roughly starting at about 18 months and ending at 7 years, wherein the child learns to communicate and uses reason in an efficient way. However, he is still inclined to intuition rather than thinking out systematically.
(iii) Concrete-operations stage:
Concrete-operations stage (from 7 to 12 years) where the child becomes capable of appreciating the constancies and develops the concept of volume but thinking is still limited in some respects.
(iv) Formal operations stage:
Formal operations stage, (from 12 years through adulthood) in which the child develops the ability to ponder and deliberate on various alternatives, and begins to approach the problem situation in a truly systematic manner.
(b) Psychosocial development:
‘Identity’ and its precedents in development are the backbone of Erikson’s psychological developmental theory. Erikson’s theory is basically an amplification of Freud’s classical psychoanalytic theory of human development. However, Erikson lays more stress on the social than the biological features in the process of development. This theory is more humanistic and optimistic, and emphasizes the importance of ‘ego’ rather than ‘id’.
Erikson postulated eight stages of development, placing more importance on adolescence (Table 28.2).
His concept of identity crises has been recognised in all the countries faced with racial, national, personal and professional problems.
Psychodynamic Model :
Recent psychodynamic model focuses on adolescent development under various dimensions
Learning Model :
Learning theory has long played an important role in understanding of human behaviour. Three major learning paradigms are: classical conditioning, operant conditioning, and observational learning. The concepts of generalization and discrimination illustrate how learning theory can account for individuality of response styles and behaviour.
Phenomenological Model :
There are different schools of approach, including the phenomenological one.
Developmental Phases of Adolescence :
I. Early Adolescence :
Early adolescence is probably the most stressful of all developmental transitions. It is generally acknowledged that within the years of age from 11 to 15, a period of rapid and drastic biological change will be experienced.
The dominant themes of early adolescence are related to the endocrine changes of puberty. There are biological changes in virtually every system of the body, including height, facial contours, fat distribution, muscular development, mood changes, and energy levels.
Early adolescence is a time of sharpest possible discontinuity with the past.
There are two major psychosocial challenges that confront early adolescents:
(1) the transition from elementary to junior high school and
(2) the shift in role status from child to adolescent.
A useful distinction has been made between “hot” and “cold” cognitions. Hot cognitions are those that are highly charged with emotion and are involved in matters of perceived threat or in situations in which cherished goals or values are in conflict or jeopardy.
There is preoccupation with body image, with deep concerns about the normality, attractiveness, and vulnerability of the changing body. Superimposed are the challenges of entry into the new social world of the high school that pose new academic and personal challenges, especially regarding friendships. The early adolescents begin to search for new behaviours, values, and reference persons and to renegotiate relationships with parents. At this time they are particularly receptive to new ideas and risk taking.
II. Middle Adolescence :
It generally encompasses the ages 15 to 17.
The middle adolescents are capable of generalizations, abstract thinking and useful introspections that can be linked to experience. As a result there is less response simply to the novel, exotic, or contradictory aspects of the environment.
The anxious bodily preoccupations of early adolescence have greatly diminished. The power of peer pressure is lessened and more differentiated judgments can now be exercised in seeking and establishing close friendship ties.
The provocative rebelliousness of the early adolescent is no longer prominent. The middle adolescent is beginning to orient more to the larger society and to learn about and to question the workings of society, politics, and government.
III. Late Adolescence :
The ages represented are 17 years through the early 20s. It represents a definitive working through of the recurrent themes of body image, autonomy, achievement, intimacy, and sense of self that, when integrated, come to embody the sense of identity.
Although there may not be a work commitment, it is a time of thoughtful educational and vocational choices that will lead to eventual economic viability. The challenge of intimacy and the establishment of a stable, mature, committed intimate relationship is perceived as critical challenge.
Essay # 4. Factors Influencing Development during Adolescence:
I. Genetic Factors :
Leaving aside major diseases clearly transmitted by genes, such as Huntington’s chorea.
Genetic influences in psychiatry are characterised by:
(a) the inheritance of traits or tendencies rather than specific abnormalities,
(b) polygenic inheritance, that is to say more than one gene being influential,
(c) the concept of threshold effects (i.e., the presence of particular genes does not mean that the characteristic they represent will be exhibited).
II. Neurological Factors :
Brain Damage:
Various degrees of injury to the brain.
Mental Retardation:
Various degrees of intellectual deficit and general mental handicap.
This may or may not be associated with brain damage, mental handicap and psychiatric problems.
Neurological disorder:
Brain disorder, including neurodegenerative disorders.
III. Constitutional and Temperamental Factors :
If by personality, it is meant that more or less characteristic, coherent and enduring set of ways of thinking and behaving that develop through childhood and adolescence, then by constitution it means those inherited (genetic) and acquired physiological qualities that underlie personality.
IV. Family and Social Influences:
(a) Attachment, separation and loss:
Early experience of disrupted or discordant family relationships, or lack of parental affection, increases the incidence of emotional and personality problems later.
(b) Parental care and control:
It is the extremes of parental behaviour, e.g. excessive permissiveness, negligence, over-protectiveness and rigid discipline which tend to be associated with many of the problems in child and adolescent development.
The parental behaviours often associated with adolescent disturbance, and which when modified can help put things right include:
1. Lack of confidence about being adult and weakness at limit-setting;
2. Parental and marital distress;
3. Inability to provide the model of a reasonably competent adult who enjoys life;
4. Difficulty in maintaining appropriate roles and boundaries;
5. Difficulty in getting the balance right between being too protective and intrusive on the one hand or negligent and uninterested on the other;
6. Giving in too readily to adolescent demands, on the one hand, or not listening to the adolescent’s point of view on the other;
7. Becoming so upset by adolescent demands that the parent becomes childishly angry and vulnerable.
(c) Parental mental disorder:
In clinical practice, parental mental illness can have impact in three main ways:
(1) When it has been a feature of family life and interacting with the child’s problems for several years past;
(2) When it interferes with the developmental tasks of adolescence, for example when a depressed parent is thereby too vulnerable to the adolescent’s challenges; and
(3) When it interferes with treatment.
(d) Parental criminal behaviour
There is a strong association between delinquency in the child and criminality in the parent, and where both parents are criminal, the association is even stronger.
Again, poor parenting skills and family discord may be important linking factors. Modelling may be another factor.
(e) Family size and structure:
Children from large families (more than 5 children) tend to show a greater incidence of conduct problems, delinquency, lower verbal intelligence and lower reading attainment.
(f) Family patterns of behaviour:
Confused or conflicting communication in families, problems in resolving arguments or making decisions, and the generation of high levels of tension do seem to be associated with child disturbance in general.
(g) Adoption, fostering and institutional care:
There is an increased rate of psychiatric disorder among adopted children, with conduct disorder among adopted boys being most prominent.
Institutional care, the placement of children and adolescents in children’s homes, is associated with a higher rate of disturbance than in the general population.
(h) The effects of schools:
Wolkind and Rutter have listed features of schools which have a positive effect on their pupils: high expectations for work and behaviour; good models of behaviour from teachers; respect for the children, with opportunities for them to take responsibilities in the school; good discipline, with appropriate praise and encouragement and sparing use of punishment; a pleasant working environment with good teacher-pupil relationships; and a good organizational structure that enables staff to work together with agreed academic and other goals.
(i) Social and transcultural influences:
Life in inner city areas seems in general to increase the rate of behaviour problems compared with small towns and rural areas. Similar influences, plus and effects on the family of immigration and unemployment and prejudice affect adolescents. Unemployment among adolescents is associated with an increase in psychiatric problems.
The effects of film and television violence have now being widely studied. There seems to be a modelling and imitative effect, particularly in younger children and among adolescents who already show conduct problems and delinquency.
Assessment:
Assessment in adolescent psychiatry requires a far wider appraisal of who is concerned about what, and who is in a position to help, than the traditional clinical diagnosis can possibly provide. See Table 28.3.
Prevalence of Disorders in the Community :
The prevalence of adolescent disorder in the community varies from place to place and with age, and depends on the criteria used. The figures given vary between around 10 and 25%. The lower end of the range is associated with younger adolescents with recognised (i.e., known to adults) psychiatric problem in more rural or sub-urban areas, and the upper figures are associated with older adolescents, with industrial and inner-city areas and with the inclusion of problems not so evident to parents and teachers.
Disorders seen in clinical practice :
Table 28.4 is a composite picture of the types of disorder likely to be seen in general psychiatric service for adolescents, and is based on data drawn from several accounts.
(a) Clinical diagnostic categories (in approximate order of frequency) :
Mood disorders:
Emotional or mixed emotional/ contact disorders, or adult-type anxiety or depressive disorders, including obsessive compulsive phobic state.
Conduct Disorders:
Hysterical disorders e.g., with paralysis and serious self-neglect.
Problems of personality development with mood and/or conduct problems, including ‘borderline’ and schizoid personality disorders, and problems of sexual identity.
Schizophrenic, Schizoaffective and affective (manic-depressive) psychoses.
Brain disorder, including epilepsy, and neurodegenerative disorder.
Anorexia nervosa and bulimia nervosa, enuresis, encopresis, and tics
(b) Changes in prevalence with age and sex:
The overall pattern seems to be a gradually increasing prevalence of psychiatric disorder from around 10% in children through 10 to 15% in mid- adolescence to around 20% in adulthood although some studies report a peak of about 20% being reached in adolescence.
In adolescence, enuresis and encopresis are less common than in earlier childhood. Hyperactivity presents less often, but children who have been hyperactive in earlier childhood sometimes present in adolescence with behavioural and other social problems.
In earlier childhood, equal numbers of girls and boys are affected by emotional disorders. In adolescence, however, as in adult life, more girls than boys are affected.
Delinquency increases markedly in adolescence and declines from early adulthood onwards.
Essay # 5. Developmental Psychopathology during the Period of Adolescence :
(a) Mood Fluctuations and Misery :
The general observation that adolescents experience a greater fluctuation of mood that adults has been demonstrated rather consistently. The feelings of transient misery and sadness reported by adolescents can be explained by several bases.
The Offer Self-image Questionnaire, administered to thousands of adolescents from 1962-1980, showed a significant upward shift of scores of depressive mood from the 1960’s to the 1970’s for both boys and girls.
Although relationships with parents may remain intact, the security experienced by identifying with the idealized parental image is sacrificed as the youth moves toward development of a separate identity.
Eventually, with the synthesis of these different value systems, the adolescent’s behaviour takes on an increasingly external and internal consistency. The wide array of conflicting societal values in regard to a youth’s engaging in sex becoming pregnant, having an abortion, bearing a child, or participating in homosexual behaviour provides numerous opportunities for remorse.
An additional factor that may draw the adolescent to a sexual relationship inspite of conflicting values is the relative emotional void produced as some distance is gained from the parent.
Among the adolescents these kinds of temporary setbacks may lead to an array of behaviours that erroneously have been termed clinical depression. These include a hypersensitivity and irritability, with a proneness to overreact to criticism. At times the adolescent may “tune out” temporarily and withdraw into a position of apathy and indifference.
At times there is a propensity to move from a passive to an active position in response to feelings of helplessness, and the adolescent may take provocative positions that elicit a punitive response from his environment. This punishment may provide a welcome relief from an immature harsh superego. For many clinicians such behaviour is summarised as adolescent turmoil.
However, the steeply rising suicide rates and the high prevalence of true adolescent depression is particularly poignant and of deep concern. It is estimated that there are 100 suicide attempts for every completed suicide. Surveys reveal that 8% to 10% of all adolescents report suicidal feelings.
(b) Sexual and Adolescent Pregnancy:
The recent significant rise in level of sexual activity among adolescents and the trend toward increasingly younger ages of initiation is well documented.
Clear documentation exists as to the biological and psychosocial risk to both mother and child in adolescent pregnancy, birth, and motherhood. The obstetrics complications, high rates of infant mortality, and perinatal morbidity have been well described. Similarly, there is excellent documentation for the social isolation, inadequate parenting skills, school drop-outs, repeat pregnancy, and chronic poverty that characterises these mothers.
(c) Developmental Issues in Drug Abuse:
If the drugs are used as a way to avoid tension and if this is done chronically, the youth’s capacity to tolerate tension and to gain in ego strength by working through stressful situations will be under developed. Drugs may thus have long term effects on important areas of ego functioning that are ordinarily developed during adolescence.
The problem behaviours of youth that are highly interrelated with regular drug use include delinquency, alcoholism, decreased school motivation and achievement, drug abuse and teenage pregnancy.
The factors associated with drug abuse can be divided into three categories:
(1) Personality factors;
(2) Social or interpersonal factors; and
(3) Sociocultural or Environmental factors.
Personal factors include an emphasis on unconventionality, rebelliousness, high risk taking, low value on achievement, and high value on autonomy. Social or interpersonal factors include alienation from parents, high influence from peers involved in problem behaviours, and little involvement in religious activities. Sociocultural factors include low social controls, disorganized environment and permissive values.
(d) Impact of Chronic Illness on Development:
During puberty, chronic illness of childhood is re-experienced as a distinct and significant adolescent phenomenon. With the major bodily changes of early adolescence and the concomitant free occupation with body image a long term illness is repraised and becomes a threat to body integrity and self-concept.
During a period typically characterized by developmental urges toward independence, the stress of illness can led to exaggerated wishes for dependence, security and nurturance on the one hand or led to denial and hyper independent, rebellious and non-compliant risk taking behaviour on the other hand. Overprotectiveness of concerned parents can aggravate any or all of these conflicts. Chronic illness may actually delay the onset of puberty.
(e) Parent-adolescent estrangement and social alienation:
Hostility and conflict with parents or substitute caregivers is a frequent presenting feature of adolescent disturbance. Parents may complain about the adolescent’s expressions of anger and defiance of unmanageable behaviour. Angry outbursts and temper tantrums occur frequently in young adolescents coping for the first time with biological changes and increasing academic and family responsibilities.
Psychiatrically disturbed adolescents, however, are likely to be involved in chronic conflict with parents who, in turn, may display psychopathology in relationships with their children, marital discord or personal psychiatric disorder.
Conflict and defiance may extend to such a serious level that there is a complete breakdown of trust and communication with parents.
(f) Anti-authority and antisocial behaviour:
Antisocial behaviour in adolescents may have arisen initially in this age-period or have continued from childhood.
Shoplifting, vandalizing public property, or spraying graffiti may occur transiently in groups of discontended teenagers who are not established delinquents.
(g) Problems in School:
The most common manifestations of adolescent disturbance in school are: disenchantment with conventional education often leading to truancy and showing other evidence of antisocial activity and conduct disorder. School refusal, usually associated with other signs of emotional disorder. Academic problems including examination anxiety, difficulties with study and academic under achievement; and disruptive behaviour, with negative attitudes towards the staff, conformity problems, bullying and association with delinquent peers.
Therapeutic Approach to Adolescent Disturbance:
Although there may be little scope or necessity for active psychiatric treatment, systematic management of interpersonal, social, educational, legal and ethical problems may be necessary and can be challenging and time consuming. These aspects of management call for full multi-disciplinary teamwork, consultation with other professionals and carefully integrated planning.
Hospitalisation and Residential Care:
Great care needs to be exercised in using residential resources, in view of the implications for adolescents of separation from home and the limited nature of residential provisions.
Psychiatric in-patient hospital treatment:
Steinberg et al have distinguished six needs to related to requests for admission, comprising the need for further work to be done with adults already involved for detailed educational reappraisal, for proper care and control, for physical containment, for an emergency safe place, for psychiatric assessment and treatment.
The role of the multidisciplinary staff and their deployment in treatment should be directed towards vigorous, short-term intervention minimizing the problems of institutionalization.
Non-psychiatric residential care of adolescents:
Disturbed adolescents may be placed in a miscellany of settings in addition to facilities administered by the National Health Service, including: schools and units for maladjusted children; independent boarding schools; children’s homes run by social service and voluntary agencies; observation and assessment centers; community homes with education, remand homes, detention centers, and borstals.
Therapeutic Work with Adolescents:
Apart from the use of antidepressant drugs in carefully selected cases of depressive disorder, the occasional use of lithium in affective psychoses and major tranquillizers in psychotic states, most adolescent disturbances can be managed without psychotropic medication.
Acute disturbance as part of personality disorder or other nonpsychotic states may warrant the use of major tranquillizers at the time of crisis, but they should not be relied upon for long term behavioural control. Hypnotics and minor tranquillizers of the Benzodiazepine group are rarely indicated and particular caution should be exercised in their prescription, in view of the scale of self- poisoning in adolescents.
The most frequent forms of individual intervention are psychotherapeutic, including behavioural techniques.
Supportive counselling, with an explicit educational component, may be indicated in the treatment.
Parental and family work:
Some form of specific work with the parents or families of disturbed adolescents is usually required and it may be an advantage to allocate a therapist to work chiefly with them.
Most adolescents are likely to accept that family sessions are an appropriate medium for dealing with issues that are public in the sense, that they impinge on all family members.
School liaison:
Information from the school or school psychological service may be essential in assessment and planned liaison about aspects of management may be useful therapeutically, as well as providing a way of monitoring progress.
Legal Aspects of Care and Community Services :
The adolescent psychiatrist needs to be familiar with all the legislation that affects adolescent patient care. In particular, it is important to be aware of the various forms of disposal for young offenders.
Related Articles:
- Disorders that are Common During Adolescence | Disorders | Psychology
- Term Paper on Adolescence | Psychology
- Physical, Cognitive & Emotional Development during Adolescence | Psychology
- Development during Childhood and Adolescence | Psychology
Adolescence , Essay , Essay on Adolescence , Psychology
- Skip to main content
- Skip to secondary menu
- Skip to primary sidebar
- Skip to footer
A Plus Topper
Improve your Grades
Adolescence Essay | Essay on Adolescence for Students and Children in English
February 13, 2024 by Prasanna
Adolescence Essay: Adolescence is the phase of transition between childhood and adulthood. It involves the physical and psychological growth and development of a person during the puberty period and is usually marked by the teenage years. The ages between 10 to 24 are generally said to be adolescence period.
During this period, the changes are associated with new risks and opportunities and are responsible for the positive and negative influences in a person’s behaviour and mindset.
You can also find more Essay Writing articles on events, persons, sports, technology and many more.
Long and Short Essays on Adolescence for Students and Kids in English
We provide students with essay samples on a long essay of 500 words and a short essay of 150 words on the topic Adolescence for reference.
Long Essay on Adolescence 500 Words in English
Long Essay on Adolescence is usually given to classes 7, 8, 9, and 10.
Adolescence is defined as the age of transformation of an individual from childhood to adulthood. The physical and psychological development and cultural expressions can start early or end later during this phase.
Adolescence starts with puberty, and bodily changes are observed during these years. In this phase, for both genders, there is a rapid increase of height and a development of sexual glands and adrenal glands with hormonal changes. The development of facial hair and deepening of voice is seen in boys. In girls, there is a development in breasts and hips at the beginning of the menstrual cycle. In these years, the bodily changes are very distinctive.
Besides, there are changes in the characteristics of the brain. The amygdala processes stress and related emotions and affect instinctual reactions and reflexes. The frontal cortex also develops, which is responsible for rational thinking, morals, judgments, and self-control. These start to develop at the onset of the adolescence period and develop over the years.
Young people experiencing the adolescence phase are exposed to various social, psychological, and behavioural changes. Individuals learn about their orientation, experience an emergence of abstract thinking and introspection. They get an idea about values, skills, coping capabilities, and the importance of a family and its values.
Various psychiatric disorders are associated with adolescence. Young girls are at greater risk for sexual and substance abuse, depression and anxiety, and sleeping and eating disorders. Boys experience a source of pride and embarrassment and various changes in their mentality, both good and bad.
In the adolescent years, there is overall cognitive development. Improvements can be observed in selective and divided attention. Both working and long-term memory are developed. The speed of registering things and self-analysis increases with self-thinking and social insight with a developed knowledge of themselves. However, there are some social constraints associated with adolescence. The social structure and stereotypical mindset often influence the mentality of a young individual. They develop resilience and are also influenced by radical and divergent ideas and changes within society.
Social developments include maintaining and developing an identity, along with cultural and belief developments. There is a sense of self-awareness and awareness towards others living in the same society. The lifestyle of an adolescent is determined by their assigned roles in the family or society in general.
Young people experiencing adolescence are often involved in physical activities like sports, dance, drama, etc., and try to find their field of interest. They find these pleasurable and gratifying. But due to academic and societal pressure, most of them cannot participate in these activities. Although very important, extra-curricular activities have been curtailed these days, restricting the individual to find exposure. The increasingly important teenagers became a driving force in music, tv shows, movies, and styling during the 1950s in many countries. In many countries, World War II’s effect has been an economic boom where teenagers used to spend money freely. In these affluent countries, teenagers have very few meaningful responsibilities, whereas, in underdeveloped countries, the young generation struggles to survive.
Short Essay on Adolescence 150 Words in English
Short Essay on Adolescence is usually given to classes 1, 2, 3, 4, 5, and 6.
Adolescence is the transition between childhood to adulthood. It involves a lot of physical, psychological, and behavioural changes. Adolescence years start with puberty. In girls, it starts at the age of 12 or 13, whereas in boys it varies from 13-15 years. Physical changes are very prominent in these years.
Adolescence and puberty have psychological and social consequences. The most important of which is looking for self-identity and improvements in cognitive abilities. Psychological changes include the development of strong viewpoints and a mentality. Social changes include self-awareness and maintaining the identity in the society a person lives in.
Generally, the years 13 -18 in an individual’s life is a period of self-discovery, confusion, and stress. During this period, a person explores his/her ability to think and act independently to survive these adolescent years.
These are the years determining how a person would turn out in the future as derived from their psychological and behavioural characteristics. They are exposed to both positive and negative influences during this period. In a few cases, adolescents chose the negative path, whereas some cannot take the mental pressure or bear with the social phobias.
10 Lines on Adolescence in English
- Adolescence is the period when a child is transformed into an adult.
- Adolescence is associated with various cognitive, physical, and psychological changes.
- It starts mostly at the age of 13, with the beginning of puberty.
- The role of hormones is very important during these years.
- Adolescence is a period in an individual’s life with specific health care and developmental necessities.
- Adolescence years are crucial as a person figures out his/her ways of managing relationships, emotions, societal, and family pressure.
- Adolescence is the period of self-discovery and self-awareness.
- The role of positive and negative influences is very important in the adolescent’s life.
- During this phase, an individual experiences new opportunity and look for exposures and grow their self-interest.
- Adolescence years are associated with improvement in the mentality and way of thinking of a young individual.
FAQ’s on Adolescence Essay
Question 1. What is the actual age of adolescence?
Answer: On average, the adolescence period starts with puberty at the age of 13-14 and continues till 24.
Question 2. What are the changes that occur in a person during adolescent years?
Answer: During adolescence, a person undergoes different physical, behavioural, and psychological changes that shape the individual.
Question 3. What are the cognitive developments that occur during adolescence?
Answer: Cognitive developments include improvements in thinking abilities, metacognition, wisdom, reflex and impulses, risk-taking actions, and self-consciousness.
- Picture Dictionary
- English Speech
- English Slogans
- English Letter Writing
- English Essay Writing
- English Textbook Answers
- Types of Certificates
- ICSE Solutions
- Selina ICSE Solutions
- ML Aggarwal Solutions
- HSSLive Plus One
- HSSLive Plus Two
- Kerala SSLC
- Distance Education
Common Problems of Adolescence: Top 10 Challenges
- Post author: Edeh Samuel Chukwuemeka ACMC
- Post published: January 15, 2023
- Post category: Scholarly Articles
Common Problems of Adolescence: Adolescence refers to a transitional stage of growth and development that occurs between childhood and adulthood. Adolescents are those between the ages of 10 and 19 according to the World Health Organization (WHO). This age range falls under WHO’s definition of young people, which includes those aged 10 to 24.
On one hand, adolescence is sometimes slightly equated with puberty and the progression of physical changes that lead to reproductive maturity in many societies whereas, the term is viewed in other areas in broader terms that go beyond the purely physical elements of maturity to include psychological, social, and moral domains. Adolescence, which is generally equated to the word teenagers in these settings, is often used to describe the time between the ages of 12 and 20.
For young people, adolescence is not an easy period since these individuals are forced to make a variety of modifications as a result of the transition to self-sufficiency. Knowing about and being prepared to address the demands and problems of this phase can go a long way to help both the parents and the young person involved. This article explores the common problems of adolescence.
Recommended: Countries with the most beautiful women in the world
Top 10 Common Challenges/Problems of Adolescence
1. Physical Changes: Changes in hormone levels cause physical changes in adolescents. Girls may first experience discomfort when their breasts grow fully. Some girls may begin to feel self-conscious about their physique. Possibly the most noticeable change that occurs throughout puberty is a boy’s voice shift and the development of facial hair. Other physical changes experienced during adolescence include:
a. The development of acne which is a serious issue
b. Muscle gain which can sometimes result in increased body weight in adolescents.
c. Both boys’ and girls’ development of pubic hair
d. Body odour becomes apparent.
e. Menstruation for girls begins.
2. Emotional changes and problems: Hormones influence an adolescent not just physically but also emotionally. Adolescents are frequently conflicted about their roles and torn between their obligations as evolving adults and their childhood aspirations.

They tend to be overly emotional (blame it on the hormones). They may get thrilled, furious, or elated about just about anything. Teenage females are prone to sobbing. Additionally, Both teenage boys and girls frequently experience mood swings, meanwhile, self-consciousness arises from physical changes. At this point, feelings of superiority or inferiority could appear. Moreover, early onset puberty might even make children feel strange.
Also see: How To Introduce Yourself To A Girl
3. Behavioural changes: Overwhelming emotions might cause impulsive conduct, which could be detrimental to the young person and other people. Typically, it’s just the usual adolescent behaviour that persists throughout that period.

a. Children gain and assert their independence during adolescence. This could lead to them challenging their parents’ rules in an argumentative way and defending what they think is correct (seen as stubbornness).
b. Adolescents are cranky, exhausted, and challenging to deal with due to significant developmental changes.
c. Adolescent males may even be driven to engage in violent altercations by their surging hormones. Additionally, they would love to listen to loud music.
d. Adolescents may desire to explore new things and take risks as a result of their newly found freedom, which can lead to reckless conduct.
e. Pressure from peers and the desire to “fit in” can sometimes cause adolescents to act in certain ways or form difficult-to-break habits.
f. Additionally, an adolescent’s appearance, sense of style, and grooming change often in ways that do not garner approval.
g. One of the prevalent behavioural problems among adolescents is lying. Adolescents may tell lies out of fear or to avoid conflict with their parents.
Recommended: Differences Between British and American English
4. Substance use and abuse: Adolescents are impressionable and readily influenced, making them particularly susceptible. Substance abuse is one of the most serious problems that parents of adolescents face across the world. One of the main reasons why they start using drugs, drinking, and smoking is peer pressure. Most adolescents try smoking or drinking before they are old enough to do so due to their propensity for taking risks. If left unchecked, what may begin as a “thrill” might develop into a habit.

Moreover, adolescents may smoke or drink because of low self-esteem and a desire to fit in. The temptation to try illegal substances may be increased by the availability of access to things like cigarettes, alcohol, narcotics, and anabolic steroids.
5. Health problems: Adolescents are both emotionally and physically vulnerable. They are prone to illnesses without sufficient dietary intake and medical care. A 2015 WHO estimate revealed that 1.3 million adolescents died in 2015, the majority from illnesses that could have been avoided.
a. Adolescents have a packed lifestyle and seldom have time to properly eat or rest since they scurry from one activity to the next. They are unable to obtain the nourishment they require due to unhealthy eating habits.
b. In girls especially, body awareness can result in eating problems. Adolescent females who obsess about their weight and attractiveness run the risk of developing anorexia or bulimia.
c. In young children, stress can also cause appetite loss and disrupted sleep.
d. Obesity can also be brought on by poor eating patterns and a sedentary lifestyle, which is often the case when adolescents consume a lot of empty calories from fast food and beverages.
Also see: Differences Between Love and Lust
6. Psychological problems: Studies have shown that over half of all mental health illnesses in adults begin at the age of 14. In fact, depression-related suicides account for one-third of all adolescent deaths. Anxiety and mood disorders are the mental health conditions that are seen most frequently in adolescents. In this age bracket, social phobias and panic disorders are prevalent.

a. Adolescents may struggle with low self-esteem or lack of confidence. Their appearance and acceptance of their body—skin colour, attractiveness, and figure—often cause them to feel inadequate or superior.
b. Low IQ and poor academic achievement might also demotivate them. They start to live their lives with a “ I’m not good enough ” mentality.
c. One of the frequent psychological issues linked to adolescence is depression.
d. Adolescent stress and pressure can result in anxiety-related problems, and mood swings can cause conduct disorder or oppositional defiant disorder.
e. Eating disorders are also psychosomatic since they begin with the adolescent having a negative self-perception and feeling the urge to alter their appearance in any way possible.
Also see: How to be a good conversationalist
7. Social problems –Dating and Relationships: Puberty is the starting point for attraction to the opposite sex. Adolescence is the period during which their sexual or reproductive organs begin to develop. Adolescents typically feel uncomfortable in social interactions at such a sensitive age. During this time, they appear to be preoccupied with engaging with friends on social networking sites, over their phones.

Furthermore, because everything appears to be happening very fast around adolescents, They face the problem of having to comprehend and accept their sexuality. Boys and girls begin to have “ strange ” sentiments toward the opposite sex and may not know how to handle them. They may feel guilty for having sex-related thoughts and sensations because they believe they are improper. Another significant component of a teen’s social life is competition. Their competitive attitude reveals a lot about their sense of self, whether that is a positive or negative one.
Also see: Best Countries For Business In The World 2023
8. Sexually Related Problems – Unplanned Pregnancy and STIs: The development of secondary sexual characteristics during adolescence gives rise to new sensations which could motivate them to experiment with their bodies.
So, adolescents who are not properly guided may become sexually active before they are ready and this could lead to unwanted pregnancies. The most serious challenge that adolescent females are posed with is unwanted pregnancy. Additionally, unprotected intercourse might result in STDs like HIV.
Also see: Oldest Sports In The World (With Pictures)
9. Addiction to cyberspace: The introduction of social media has altered how we communicate with one another. In the lives of adolescents, this is another common problem that affects them. Most adolescents are hooked to the internet, and typically these ones have fewer friends and are less involved in social activities.
They lead isolated lifestyles and are content to spend hours online. Their physical activity is also reduced due to addiction to the internet, leading to an unhealthy and sedentary lifestyle. Let’s not forget, academic performance is also negatively impacted by internet addiction.
10. Aggression and violence: Adolescent males are particularly vulnerable to aggression. As the males begin to bulk up, get taller, and have a manlier voice, they are also sensitive, irritable, and prone to letting people get on their nerves. So, we see boys in their adolescence might get into fights at school.
But that’s not all, a common problem seen in adolescence is bullying which is a serious issue that both males and girls struggle with. As shown in a WHO estimate, interpersonal violence accounts for around 180 adolescent mortality worldwide.
Recommended: Toughest animals in the world currently
Adolescents undergo a variety of changes as they go through the transition from childhood to adulthood. A young person’s life at this point is also quite delicate since they might be dealing with several issues related to adolescence.

Edeh Samuel Chukwuemeka, ACMC, is a lawyer and a certified mediator/conciliator in Nigeria. He is also a developer with knowledge in various programming languages. Samuel is determined to leverage his skills in technology, SEO, and legal practice to revolutionize the legal profession worldwide by creating web and mobile applications that simplify legal research. Sam is also passionate about educating and providing valuable information to people.

- Subscribe to journal Subscribe
- Get new issue alerts Get alerts
- Submit a Manuscript
Secondary Logo
Journal logo.
Colleague's E-mail is Invalid
Your message has been successfully sent to your colleague.
Save my selection
Adolescent Mental Health
Issues, challenges, and solutions.
Nebhinani, Naresh; Jain, Shreyance
Department of Psychiatry, All India Institute of Medical Science, Jodhpur, Rajasthan, India
Address for correspondence: Dr. Naresh Nebhinani, Department of Psychiatry, All India Institute of Medical Science, Jodhpur - 342 005, Rajasthan, India. E-mail: [email protected]
Adolescence is a transition phase from childhood to adulthood, which is marked by several biological, cognitive, and psychosocial changes. The characteristics which emerge during adolescence involve: a tendency to experiment and seek novel experiences, a heightened sense of vulnerability, a low risk perception, an intense desire for independence, and an inner search for self-identity which gradually shape up their personality throughout the developing years. It is a critical period characterized by neurobiological and physical maturation leading to enhanced psychological awareness and higher level of social and emotional interactions with peers and adults. From neurobiological perspective also adolescents can be viewed as “works in progress,” with academic, interpersonal, and emotional challenges, and exploring new territories using their talents, and experimenting with social identities.[ 1 ] On one hand, it is a phase of tremendous growth in preparation of adults' roles and skills to sustain pressures and challenges, whereas on the other, it is transition phase that can increase risk of various psychological disorders, adjustment problems, and suicide.[ 2 ] Positive and promotive mental health in this period ensures a smooth progress to later adult life.[ 3 ]
ADOLESCENT PSYCHIATRIC BURDEN
Worldwide, it is estimated that 10%–20% of adolescents' experience mental health conditions, yet the majority of times, it remains underdiagnosed and undertreated. Signs of poor mental health are overlooked for several reasons, such as a lack of knowledge or awareness of mental health among health workers and also the stigma that prevent from seeking help.[ 4 ] According to the 2011 census, around one-fourth of the Indian population is adolescent (253 million).[ 5 6 ] As per the National Mental Health Survey of India (2015–2016), the prevalence of psychiatric disorders among adolescents (13–17 years) is reported around 7.3%.[ 7 ] Yet, very little attention has been paid to the mental health issues of this age group.
DIMENSIONS OF MENTAL HEALTH PROBLEMS
The prevalence and pattern of mental and behavioral disorders show a change during adolescence. The mental health need of this population group is distinct from both children and adults. Nearly 50% of adult psychiatric disorders begin before the age of 14 years.[ 3 ] Preexisting psychiatric disorders during childhood may act as predisposing or precipitating factor for mental illness during the adolescent period. These impairing psychiatric disorders emerge in approximately 20% of the adolescent population.[ 1 ]
MAJOR PSYCHIATRIC DISORDERS IN ADOLESCENCE
Depressive disorders become more prevalent, behavioral disturbances, such as suicidality, eating disorders, and substance abuse, begin to emerge in these years. The prevalence rates increase from 1% to 2% in childhood to around 10%–20% by late adolescence, similar to adults.[ 8 ] Depression and stress are more prevalent among school-going adolescent girls. Approximately 40%–90% of adolescents with depression have a comorbid psychiatric disorder such as anxiety disorders, conduct disorders, substance abuse, and personality disorders in the case of adolescents.[ 8 9 ] Anxiety disorders are also commonly encountered among the adolescent population.[ 10 ] In India, suicide is a leading cause of death among young people as 25% of deaths in adolescent boys and 50%–75% of deaths in adolescent girls is due to suicide. Every hour, one student commits suicide in India, according to the National Crime Records Bureau report in 2015.[ 2 ] Community surveys suggest that tobacco and alcohol are prevalent substances of abuse among Indian adolescents. The experimentation with “gateway” drugs such as tobacco, alcohol, and inhalants may lead to indulgence in high-risk behaviors. The substance use has spread to different areas of the world, including India and increasing in adolescents' age groups even in the distant regions. In this issue, Majumder et al .[ 5 ] and Keyho et al .[ 6 ] have assessed psychiatric morbidity in adolescent patients and school-going adolescents in North-Eastern India. Majumder et al . have assessed psychiatric morbidity in 474 consecutive adolescent patients (10–19 years) attending to psychiatric services at tertiary care center in Manipur and reported the most common disorder as neurotic, stress-related, and somatoform disorders (41%), followed by psychotropic substance use disorders (21%) (including opioid dependence in 14% and cannabis dependence in 3% of adolescent).[ 5 ] While the most common disorder was substance use disorders (37%) in adolescent boys, and neurotic, stress-related, and somatoform disorders (61%) in adolescent girls.[ 5 ] Keyho et al . have assessed the mental health status of 702 school-going adolescents (13–19 years) in Kohima and reported emotional problems in 17%, hyperactivity in 16%, and conduct problem in 15%.[ 6 ]
Another issue which needs focus and active intervention is sexual abuse which has long been the subject of the study in the field of mental and social health. Nearly one-third of higher secondary school-going adolescents reported experiencing some form of sexual abuse over the past 12 months and 6% reported experiencing forced sex.[ 8 ] The Internet and social media are ubiquitous among adolescents and serve as platforms to socialize and to communicate. The “digital revolution” has highlighted the adaptive nature of the adolescent brain in its ability to incorporate these technologies. Reports had also indicated that about 90% of adolescents use the Internet in many ways, including messaging, blogging, posting photos, videos, and stories.[ 1 ] Positive effects of the Internet identified for adolescents include increased communication, increased access to academic information, and familiarity with social and cultural habits of people worldwide. On the other side, pathological Internet use/Internet addiction is reported high in Indian schools (prevalence of 11.8%) and college settings (prevalence of 42.9%). The consequences of these are manifold ranging from alteration of biological functions, substance use to self-harm, and even death.[ 11 ]
FACTORS AFFECTING THE PSYCHOLOGICAL HEALTH OF INDIAN ADOLESCENTS
There is a complex biopsychosocial framework of risk factors operating in the lives of adolescents which include self, home, school, peer group, and neighborhood which may be associated with the mental health disorder.[ 1 8 ] Risk factors include all variables that increase the probability that a given child or adolescent will develop psychopathology while protective factors decrease the risk of developing psychopathology. Rarely, a single-risk-factor accounts for the emergence and inhibition of a psychiatric disorder.[ 1 12 ] There is a significant effect of the following factors on the mental health of adolescents: recent sociocultural changes, poor social support, the breakdown of extended and joint families, the ambiguity of societal values, and increasing gap between aspirations and possible achievements, substance abuse, etc.[ 5 12 13 ]
BARRIERS IN THE SERVICE DELIVERY
Stigma about mental health and lack of education and awareness forms one of the factors for seeking psychiatric consultation. Above that beliefs about mental illnesses influence help-seeking attitudes and patterns in people. In India, only one-third of the families (37.5%) of children and adolescents with mental disorders perceived that their children had any psychiatric problem.[ 14 ] At the stakeholder levels limitations of the existing policies and programs, the lack of alignment across them and the fragmentation of governance of adolescent mental health between ministries and departments, are likely to pose major barriers to their effective and efficient implementation.[ 15 ]
INTERVENTIONS FOR PSYCHIATRIC DISORDERS IN YOUTH: PROPOSED SOLUTIONS
There is a need for a special emphasis on adolescent mental health at different levels with coordinated efforts. To strengthen child and adolescent mental health care in a country, it should be supported by the necessary policies, programs, legislation, policy, budget, primary-care system, training programs, and service delivery system.[ 16 ] Interventions to address psychiatric disorders in youth are universal, targeted, and clinical. Universal interventions also termed primary prevention, are received by all children and families within a specific geographical distribution. There is potential scope for primary or preventive interventions at this age. Targeted interventions are designed for children at increased risk for psychiatric disorders and Clinical interventions provide treatment to adolescent with psychiatric disorder which includes psychosocial, psychopharmacological, and other environmental interventions.[ 17 18 ] Preventive efforts not only improve the mental health of young but also may have far-reaching consequences in reducing adult psychiatric morbidity.[ 12 ]
ROLE OF PARENTS AND TEACHERS
Schools and colleges may play a vital role in the development of adolescents and provide a room and scope for intervention. Family as an institution continues to play a large role in influencing adolescents across all sections of the society in India. Parental support and healthy parenting have been identified as contributors to better mental health outcomes and reduction in help-seeking barriers in their children.[ 19 ] Sensitization and training of teachers and counselors to handle adolescent mental health issues can further help in early identification of mental health problems. Drug awareness campaigns should be regularly conducted in schools and colleges with the facility of screening in the high-risk population.[ 3 ] There should be a focus on enhancing social skills to resist peer pressure and the ability to say “no” to drugs. Special attention should be devoted to children with scholastic difficulties or poor academic achievements with an encouraging and supportive approach. Resilience-focused interventions such as capacity building strategies, and coping skills may be designed to enhance resilience thereby positively influencing mental health.[ 20 ] Interventions such as “health education” pertaining to adolescent health, sex education, and pubertal changes have shown improvement in knowledge among adolescent girls.[ 21 ] Model-based health delivery approaches such as mental health promotion such as yoga, life skills approach in secondary schools has shown significant results and can be further strengthened.[ 22 23 24 ]
COLLABORATIVE ROLE OF HEALTH PROFESSIONALS
Skilled and competent workforce is need of the hour, especially in dealing with adolescent mental health at various levels. Professionals such as physicians, pediatricians, and nurses can be trained in relevant aspects of adolescent mental health promotion and preventive activities. The key to good liaison is the better understanding of respective roles and responsibilities by each professional of the multidisciplinary team.[ 8 ] With development of effective linkages along with adequate referral system may further help in management of priority mental health disorders in children and adolescents and dealing with emergency conditions like suicide. There is also a need to build on indigenous ways of child and adolescent health promotion. Computer-assisted interventions may be employed, especially for urban adolescents.[ 15 ] Policies and programs need to be better aligned with evidence-based practices emerging from both scientific studies and experience with the regular update of practice guidelines will further help in increasing the competence in this direction.[ 25 ]
NEED FOR EFFECTIVE INTER-SECTORAL LINKAGES AND PUBLIC HEALTH APPROACH
There is a need to develop effective inter-sectoral linkages comprising the educational, legal and juvenile justice system, social welfare, and voluntary organizations and nongovernmental organizations with more effective linkage of adolescent mental health with the national programs such as National Rural Health Mission and the Reproductive and Child Health Programme.[ 8 ]
Seeing the huge-dimensional problem development of community and primary health can be a feasible, acceptable, and affordable approach for catering to the mental health needs of Indian children.[ 26 27 ] This may be achieved through mobile health camps, regular screening and health check-ups like other medical morbidities at primary levels with the involvement of Anganwadi workers or primary care clinics under district mental health program.[ 3 ] It is important to establish a body at center and state levels to have an effective mechanism for coordination and monitoring of services to facilitate an effective liaison with different organizations on adolescent mental health issues.[ 3 8 ]
To conclude, child and adolescent mental health is a shared responsibility. For any interventions to be effective, there is a need for synergy between different stakeholders. Adolescents having mental health problems and disorders, need to have access to timely, integrated, high-quality, multi-disciplinary mental health services to ensure effective assessment, treatment, and support. The preservation and promotion of mental health in the young population have conventionally been viewed as an individual or family responsibility; however, it is important to emphasize it at a much broader level. There is a need to promote the concept of positive health with public health approaches including expansion of the community services for mental disorders.[ 3 12 ] There is an urgent need to explore newer models of service delivery apart from standard models of hospital-based care. The newer service delivery models should incorporate cross-cultural, multilingual, and multiregional requirements. A positive step in this direction could be the formulation of mental health policy specifically for the younger population to provide a developmental framework to enhance adolescent mental health.
- Cited Here |
- Google Scholar
- PubMed | CrossRef |
- View Full Text | PubMed | CrossRef |
- + Favorites
- View in Gallery
Being a teen comes with exciting milestones that double as challenges – like becoming independent, navigating high school and forming new relationships. For all the highs that come with getting a driver’s license or acing that difficult test, there are lows that come with growing up in a rapidly changing world being shaped by the COVID-19 pandemic, social media and distance learning.
Teens’ brains are growing and developing, and the ways they process their experiences and spend their time are crucial to their development. Each great experience and every embarrassing moment can impact their mental health.
Sometimes a mood is about more than just being lonely or angry or frustrated.
Mental health challenges are different than situational sadness or fatigue. They’re more severe and longer-lasting, and they can have a large impact on daily life. Some common mental health challenges are anxiety, depression, eating disorders, substance use, and experiencing trauma. They can affect a teen’s usual way of thinking, feeling or acting, and interfere with daily life.
Adding to the urgency: Mental health challenges among teens are not uncommon. Up to 75% of mental health challenges emerge during adolescence, and according to the Mental Health First Aid (MHFA) curriculum, one in five teens has had a serious mental health disorder at some point in their life.
Not every mental health challenge will be diagnosed as a mental disorder, but every challenge should be taken seriously.
A mental health challenge left unchecked can become a more serious problem that also impacts physical health — think of how substance use, and changes in sleep patterns and eating habits affect the body as well as the mind. Signs of fatigue, withdrawing socially or changes in mood may point to an emerging mental health challenge like a depressive or substance use disorder.
As teens mature, they begin spending more time with their friends, gain a sense of identity and purpose, and become more independent. All of these experiences are crucial for their development, and a mental health challenge can disrupt or complicate that development. Depending on the severity of the mental health challenge, the effects can last long into adulthood if left unaddressed.
How do we address teens’ mental health?
Teens need tools to talk about what’s going on with them, and they need tools for when their friends reach out to them. Research shows that teens are more likely to talk to their friends than an adult about troubles they’re facing.
That’s why it’s important to talk to teens about the challenges they may deal with as they grow up and navigate young adulthood. They need to know it’s OK to sometimes feel sad, angry, alone, and frustrated. But persistent problems may be pointing to something else, and it is crucial to be able to recognize early warning signs so teens can get appropriate help in a timely manner. teen Mental Health First Aid teaches high school students in grades 10-12 how to identify, understand and respond to signs of a mental health problem or crisis among their friends — and how to bring in a trusted adult when it’s appropriate and necessary. With proper care and treatment, many teens with mental health or substance use challenges can recover. The first step is getting help.
Learn more about teen Mental Health First Aid by watching this video and checking out our blog . Your school or youth-serving organization can also apply to bring this training to your community.
teen Mental Health First Aid is run by the National Council for Mental Wellbeing and supported by Lady Gaga’s Born This Way Foundation.
Resource Guide:
- Mental Health First Aid USA. (2020). teen Mental Health First Aid USA: A manual for young people in 10 th -12 th grade helping their friends. Washington, DC: National Council for Mental Wellbeing.
National Institute of Mental Health. (2020). The Teen Brain: 7 Things to Know. U.S. Department of Health and Human Services, https://www.nimh.nih.gov/health/publications/the-teen-brain-7-things-to-know/index.shtml.
Get the latest MHFA blogs, news and updates delivered directly to your inbox so you never miss a post.
Share and help spread the word.
Related stories.
No related posts.
Warning: The NCBI web site requires JavaScript to function. more...

An official website of the United States government
The .gov means it's official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you're on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- Browse Titles
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Division of Behavioral and Social Sciences and Education; Board on Children, Youth, and Families; Committee on the Neurobiological and Socio-behavioral Science of Adolescent Development and Its Applications; Backes EP, Bonnie RJ, editors. The Promise of Adolescence: Realizing Opportunity for All Youth. Washington (DC): National Academies Press (US); 2019 May 16.

The Promise of Adolescence: Realizing Opportunity for All Youth.
- Hardcopy Version at National Academies Press
2 Adolescent Development
A dolescence is a period of significant development that begins with the onset of puberty 1 and ends in the mid-20s. Consider how different a person is at the age of 12 from the person he or she is at age 24. The trajectory between those two ages involves a profound amount of change in all domains of development—biological, cognitive, psychosocial, and emotional. Personal relationships and settings also change during this period, as peers and romantic partners become more central and as the adolescent moves into and then beyond secondary school or gains employment.
Importantly, although the developmental plasticity that characterizes the period makes adolescents malleable, malleability is not synonymous with passivity. Indeed, adolescents are increasingly active agents in their own developmental process. Yet, as they explore, experiment, and learn, they still require scaffolding and support, including environments that bolster opportunities to thrive. A toxic environment makes healthy adolescent development challenging. Ultimately, the transformations in body, brain, and behavior that occur during adolescence interact with each other and with the environment to shape pathways to adulthood.
Each stage of life depends on what has come before it, and young people certainly do not enter adolescence with a “blank slate.” Rather, adolescent development is partly a consequence of earlier life experiences. However, these early life experiences are not determinative, and the adaptive plasticity of adolescence marks it as a window of opportunity for change through which mechanisms of resilience, recovery, and development are possible. ( Chapter 3 discusses this life-course perspective on development in detail.) This chapter explores three key domains of adolescent development: puberty, neurobiological development, and psychosocial development. Within each domain, we highlight processes that reflect the capacity for adaptive plasticity during adolescence and beyond, marking adolescence as a period of unique opportunity for positive developmental trajectories.
Puberty, a normative developmental transition that all youth experience, is shaped by both social and biological processes. Although often misconstrued as an abrupt, discrete event, puberty is actually a gradual process occurring between childhood and adolescence and one that takes many years to complete ( Dorn and Biro, 2011 ). Biologically, puberty involves a series of complex alterations at both the neural and endocrine levels over an extended period that result in changes in body shape (morphology), including the maturation of primary and secondary sex characteristics during late childhood and early adolescence and, ultimately, the acquisition of reproductive maturity ( Dorn and Biro, 2011 ; Natsuaki et al., 2014 ).
Two biological components of puberty, adrenarche and gonadarche , are relevant in understanding the link between puberty and adolescent wellbeing. Adrenarche, which typically begins between ages 6 and 9, refers to the maturation of the hypothalamic-pituitary-adrenal (HPA) axis, during which the levels of adrenal androgens (e.g., dehydroepiandrosterone and its sulfate) begin to increase. While adrenarche begins in late childhood, levels of adrenarchal hormones continue to rise throughout adolescence, peaking in the early 20's ( Blakemore et al., 2010 ). Adrenal androgens contribute to the growth of pubic and axillary hair. Gonadarche typically begins in early adolescence, at approximately ages 9 to 11, and involves the reactivation of the hypothalamic-pituitary-gonadal (HPG) axis (for a review, see Sisk and Foster, 2004 ). 2 The rise of gonadal steroid hormones to adult levels occurs as a result of HPG reactivation and is primarily responsible for breast and genital development in girls.
The consequence of these complex changes in HPA and HPG axes at the neuroendocrine level is a coordinated series of visible, signature changes in body parts. These include a growth spurt, changes in skin (e.g., acne) and in body odor, the accumulation of body fat (in girls), the appearance of breast budding (in girls) and enlargement of testes and increased penis size (in boys), the growth of pubic and axillary hair, the growth of facial hair (in boys), and the arrival of the first period (i.e., menarche, in girls). Key pubertal events are highlighted in Figure 2-1 ; however, as discussed next, there is a great deal of variation in the timing and tempo of these events.
Key pubertal events across adolescence.
It is useful to distinguish three distinct yet interrelated ways to conceptualize individual differences in pubertal maturation. Pubertal status refers to how far along adolescents are in the continuum of pubertal maturation at any given moment. For instance, if an 11-year-old girl has just experienced menarche, she is considered to have advanced pubertal status because menarche is the last event that occurs in the process of the female pubertal transition. Pubertal status is inherently confounded with age, because older adolescents are more likely to have attained advanced pubertal status.
Pubertal timing , on the other hand, refers to how mature an adolescent is when compared to his or her same-sex peers who are of the same age. In other words, pubertal timing always includes a reference group of one's peers. For example, a girl who experiences menarche at age 10 may be an earlier maturer in the United States, because her menarcheal timing is earlier than the national average age for menarche nationwide, which was found to be 12.4 years in a cohort of girls born between 1980 and 1984 ( McDowell et al., 2007 ). Only 10 percent of girls in the United States are estimated to have experienced menarche before 11.11 years of age ( Chumlea et al., 2003 ), suggesting that the girl in this example would be considered to have early pubertal timing. Unlike pubertal status, pubertal timing is not confounded by age because, by definition, pubertal timing is inherently standardized within same-sex, same-age peers typically residing in the same country.
Pubertal tempo is a within-the-individual metric that refers to how quickly a person completes these sets of pubertal changes. For example, some boys may experience a deepening of their voice and the development of facial, axillary, and pubic hair all within a matter of months, whereas other boys may have a gap of several years between voice-deepening and the development of facial hair. Pubertal tempo has gained more attention recently with the rise of sophisticated longitudinal methodology and the resulting availability of longitudinal data on pubertal maturation (e.g., Ge et al., 2003 ; Marceau et al., 2011 ; Mendle et al., 2010 ).
Regardless of the metric used, most of the research on adolescent pubertal development has focused on girls. We know comparatively little about the processes, correlates, and outcomes of pubertal maturation in boys, except for the well-replicated findings that girls typically begin and complete puberty before boys. Evidence is now emerging that the relationship between puberty and structural brain development in the amygdala and hippocampus region may differ by sex ( Satterthwaite et al., 2014 ; Vijayakumar et al., 2018 ). These sex differences in associations between brain development and puberty are relevant for understanding psychiatric disorders characterized by both hippocampal dysfunction and prominent gender disparities during adolescence.
It is also important to consider the pubertal development of transgender and gender-nonconforming youth. Transgender and gender-nonconforming individuals usually identify as a gender other than the one they were assigned at birth ( Sylvia Rivera Law Project, 2012 ). Individuals who are gender-nonconforming may identify as transgender, genderqueer, gender-fluid, gender-expansive, or nonbinary. Puberty is a time that can be enormously stressful, and the fear of developing—or the actual development of—secondary sexual characteristics that do not match a child's gender identity can be intense and even destabilizing ( de Vries et al., 2011 ). Some transgender and gender-nonconforming youth might take medications that block puberty. Although puberty blockers have the potential to ease the process of transitioning, the long-term health effects of these drugs are not yet known ( Boskey, 2014 ; Kreukels and Cohen-Kettenis, 2011 ).
The Role of Early Experiences on Pubertal Timing and Tempo
As noted earlier, the timing and rate of pubertal development vary greatly. The age at which someone matures is due to a combination of genetic and environmental influences (e.g., Mustanski et al., 2004 ). Early life experiences, including social risks and disadvantages, have been shown to accelerate pubertal tempo and lower the age of pubertal timing ( Marshall and Tanner, 1969 ). Specifically, accelerated pubertal tempo and early pubertal timing have been associated with stressors, including childhood sexual abuse and physical abuse, obesity, prematurity, light exposure, father absence, and exposure to endocrine disruptors (such as chemicals in plastics, pesticides, hair-care products, and many meat and dairy items) (see e.g., Steinberg, 2014 , pp. 54–55). This section reviews the literature on associations between these early experiences and normative variations in pubertal timing and tempo. We close this section with a brief discussion of these associations as a marker of adaptive plasticity.
Maltreatment
One of the most widely studied early experiences related to pubertal development is child maltreatment, and in particular, sexual abuse. A series of studies shows that the age of menarche tends to be lower for girls who experienced child sexual abuse as compared to girls who have not experienced this ( Bergevin et al., 2003 ; Natsuaki et al., 2011 ; Romans et al., 2003 ; Turner et al., 1999 ; Wise et al., 2009 ). Trickett and Putnam (1993) suggested that the trauma of child sexual abuse introduces physiological as well as psychological consequences for children, including accelerated maturation by premature activation of the HPA and HPG axes. In addition, some studies have observed a relationship between childhood physical abuse and early maturation, though less robustly and less consistently than for sexual abuse ( Bergevin et al., 2003 ; Wise et al., 2009 ), and these studies do not always control for the possibility of concurrent sexual abuse (e.g., Romans et al., 2003 ).
In one of the few studies to examine pubertal development longitudinally in adolescents with maltreatment histories, Mendle and colleagues (2011) followed a sample of 100 girls in foster care at four points in time over 2 years, beginning in the spring of their final year of elementary school. The previously established association between sexual abuse and earlier onset of maturation and earlier age at menarche was replicated, and in addition, physical abuse was found to be related to a more rapid tempo of pubertal development. A recent longitudinal study of 84 sexually abused girls and matched-comparison girls replicated the association between sexual abuse and earlier pubertal onset (including breast development and pubic hair; Noll et al., 2017 ). Further, using this same sample, childhood sexual abuse predicted earlier pubertal development which, in turn, was associated with higher levels of internalizing symptoms such as depression and anxiety concurrently and 2 years later ( Mendle et al., 2014 ). A third study with this sample found that earlier-maturing girls were more anxious in the pre- and peri-menarche periods than their later-maturing peers; however, their anxiety declined after menarche, suggesting a time-limited effect on mental health and the potential for recovery upon completion of pubertal maturation, as girls enter later adolescence ( Natsuaki et al., 2011 ).
The association between sexual abuse and earlier pubertal development was recently replicated using a large population-based sample of adolescents, the National Longitudinal Study of Adolescent Health 3 ( N = 6,273 girls). In that study, child sexual abuse predicted earlier menarche and development of secondary sexual characteristics, whereas other types of maltreatment did not ( Mendle et al., 2016 ). The distinctive role for early pubertal timing suggests that the heightened sexual circumstances of puberty may be especially challenging for girls whose lives have already been disrupted by adverse early experiences, yet also suggests a potential opportunity for intervention and resilience, particularly in later adolescence, once pubertal development is complete. However, the vast majority of research in this area has focused solely on girls, and we know very little about whether maltreatment is also associated with earlier pubertal timing in boys.
Other Family and Health Factors
Other family factors that may be stress-inducing yet much less extreme than maltreatment have also been associated with pubertal timing and tempo. For example, Quinlan (2003) found that the number of caretaking transitions a child experiences was associated with earlier menarche. Sung and colleagues (2016) found that exposure to greater parental harshness (but not unpredictability) during the first 5 years of life predicted earlier menarche; and a recent meta-analysis found that father absence was significantly related to earlier menarche ( Webster et al., 2014 ), although genetic confounding may play a role in this association ( Barbaro et al., 2017 ).
Health factors that may affect the metabolic system are also predictive of pubertal timing. For example, in girls, low birth weight ( Belsky et al., 2007 ) and obesity/higher body mass index (BMI) ( Wagner et al., 2015 ) have both been associated with earlier pubertal maturation. For boys, overweight (BMI ≥ 85th and < 95th percentile) has been associated with earlier pubertal maturation, whereas obesity (BMI ≥ 95th percentile) was associated with later pubertal maturation ( Lee et al., 2016 ), suggesting a complex association between aspects of the metabolic system and puberty in boys.
Environmental Exposures
Recently, researchers have examined whether a child's exposure to chemicals is related to pubertal maturation by serving as an endocrine disruptor (see e.g., Lomniczi et al., 2013 ; Simonneaux et al., 2013 ; Steingraber, 2007 ). In the first longitudinal study of age of pubertal timing and exposure to persistent organic pollutants—chemicals used in flame retardants—researchers found that the age at pubertal transition was consistently older in participants who were found to have higher chemical concentrations in collected blood samples ( Windham et al., 2015 ). The effects of neuroendocrine disruptors on girls' pubertal timing may begin during the prenatal period, as there is evidence that female reproductive development is affected by phthalate or bisphenol A exposure during specific critical periods of development in the mother's uterus ( Watkins et al., 2017 ).
Accelerated Maturation and Adaptive Plasticity
It is clear that early experiences can factor into accelerated pubertal timing and tempo, and theorists suggest that this may be adaptive. According to Mendle and colleagues (2011, p. 8) , “age at certain stressful life transitions represents a dose-response relationship with maturation, with earlier ages at these events associated with earlier development (e.g., Ellis and Garber, 2000 ).” Belsky et al. (1991) posited that children who are raised in harsh, stressful environments may have accelerated pubertal development to compensate for a mistrust of commitment and of investment in social relationships. According to Belsky and colleagues, early pubertal timing may serve the evolutionary biological purpose of elongating the window for reproductivity and fertility, to permit more conceptions in a lifetime. Thus, the well-documented association between adverse early life experiences and early pubertal development may itself be an adaptive response, one that reflects the plasticity in neurobiological systems during adolescence to adapt to the specific socio-cultural context.
The Social Context of Pubertal Maturation
Despite the role that stressful early life events play in accelerating pubertal timing, it is important to note that adolescence is also a period of potential for recovery. Even when an adolescent has experienced early adversity and this has precipitated earlier pubertal maturation, the social context in which that adolescent is developing can ultimately change the trajectory of their outcomes—for better or worse. For example, closer and less conflict-laden parent-child relationships can reduce associations between pubertal maturation and behavior problems, while more conflict-laden and less close relationships exacerbate them ( Booth et al., 2003 ; Dorn et al., 2009 ; Fang et al., 2009 ). Parental knowledge of an adolescent child's whereabouts and activities also plays a role, as the influence of pubertal timing on problematic outcomes is weakened when such parental knowledge of adolescent whereabouts and activities is high, and it is amplified when knowledge is low ( Marceau et al., 2015 ; Westling et al., 2008 ). During early childhood, a secure infant-mother attachment can buffer girls from the later effects of harsh environments on earlier pubertal maturation ( Sung et al., 2016 ).
The Context of Biological Sex and Gender Norms
The biological changes of puberty take place in social and cultural contexts, and these dynamic person-context interactions have implications for adolescent development. For instance, the physical changes associated with pubertal maturation affect an adolescent's self-image as much as the way he or she is treated and responded to by others ( Graber et al., 2010 ), and culturally grounded gender norms may make these associations more salient for girls than boys. Indeed, in the United States, although menstruation is acknowledged as a normal biological event, it is nevertheless often accompanied by feelings of shame and the need to conceal it from others, particularly males ( Stubbs, 2008 ). As a result, the arrival of a girl's first menstrual cycle is often accompanied by embarrassment and ambivalence ( Brooks-Gunn et al., 1994 ; Moore, 1995 ; Tang et al., 2003 ), as well as by negative feelings ( Rembeck et al., 2006 ), including anxiety, surprise, dismay, panic, and confusion ( Brooks-Gunn and Ruble, 1982 ; Ruble and Brooks-Gunn, 1982 ).
The arrival of puberty has other social consequences, such as changing dynamics and maturing relationships with parents, siblings, and peers, as well as the emergence of peer relationships with adults. Pubertal maturation is associated with a higher incidence of sexual harassment, both by peers of the same gender and across genders ( McMasters et al., 2002 ; Petersen and Hyde, 2009 ; Stattin and Magnusson, 1990 ). Social consequences may be exacerbated among youth experiencing early pubertal timing.
The increase in pubertal hormones (e.g., estradiol, progesterone, testosterone, dehydroepiandrosterone) and the changes they drive, such as the emergence of secondary sex characteristics, is also associated with the development of substance use ( Auchus and Rainey, 2004 ; Grumbach, 2002 ; Grumbach and Styne, 2003 ; Havelock et al., 2004 ; Matchock et al., 2007 ; Oberfield et al., 1990 ; Terasawa and Fernandez, 2001 ; Young and Altemus, 2004 ). At the same time, the causal direction of these findings is somewhat mixed ( Castellanos-Ryan et al., 2013 ; Dawes et al., 1999 ; Marceau et al., 2015 ), with variation by sex. In girls, relatively early pubertal timing and faster pubertal tempo often mark an increased risk for adolescent substance use ( Cance et al., 2013 ; Castellanos-Ryan et al., 2013 ; Costello et al., 2007 ; Lee et al., 2014 ). By contrast, in boys later pubertal timing and/or slower pubertal tempo mark an increased risk for substance use ( Davis et al., 2015 ; Marceau et al., 2015 ; Mendle and Ferrero, 2012 ). This striking gender difference in associations between pubertal maturation and substance use highlights how the same biological event (pubertal maturation) can lead to very different outcomes as a function of one's biological sex.
Puberty and Stress Sensitivity
Puberty-related hormones influence the way adolescents adjust to their environment, for example by experiencing symptoms of depression and anxiety. One mechanism through which this might occur is in pubertal hormones' ability to alter sensitivity to stress, making adolescent girls particularly sensitive to exogenous stressors. Recent studies using salivary cortisol as an index of stress regulation have documented heightened stress reactivity and delayed post-stress recovery in pubescent adolescents ( Gunnar, et al., 2009 ; Stroud et al., 2004 ; Walker et al., 2004 ). Cortisol is a steroid hormone released by the HPA axis, and disruption to this axis has been implicated in the development of symptoms of depression and anxiety (e.g., Gold and Chrousos, 2002 ; Guerry and Hastings, 2011 ; Sapolsky, 2000 ).
In fact, cortisol secretion is closely intertwined with age, puberty, and sex, which together appear to contribute to adolescent girls' vulnerability to external stressors ( Walker et al., 2004 ; Young and Altemus, 2004 ). As will be discussed in Chapter 3 , cortisol, along with neuroendocrine, autonomic, immune, and metabolic mediators, usually promotes positive adaptation in the body and the brain, such as efficient operation of the stress response system. However, when cortisol is over- or under-produced it can, along with the other mediators, produce negative effects on the body and brain, such as forming insulin resistance and remodeling the brain circuits that alter mood and behavior. At the same time, as will be shown in Chapter 3 , interventions during adolescence have the potential to mediate the harmful effects of stress.
In summary, puberty is shaped by both biological and social processes. Biologically, puberty occurs over an extended period during which neuroendocrine alterations result in the maturation of primary and secondary sex characteristics and the acquisition of reproductive maturity. The timing and tempo of pubertal development varies greatly, and the age at which an adolescent matures depends upon a combination of genetic and environmental influences, including early life experiences. Socially, pubertal maturation and its accompanying physical changes affect how adolescents perceive themselves and how they are treated by others, and early pubertal timing especially has been shown to have social consequences. While we know a great deal about the biological processes of puberty, much of the research, particularly on the role of adverse early experiences, is based on studies of girls rather than boys and excludes transgender and gender-nonconforming youth. Thus, it is important to monitor whether or not conclusions drawn from the extant research are relevant for both girls and boys, and to consider how further study of puberty in boys, transgender youth, and gender-nonconforming youth may deepen our understanding of these dynamic processes.
Despite this limitation, research on associations between stress exposure and pubertal timing and tempo makes clear the importance of early experiences and highlights the role of social determinants of health. Stressful living conditions are related to earlier pubertal timing and accelerated pubertal tempo. While early puberty may be an evolutionarily adaptive response to context that reflects neurobiological plasticity, there are important consequences that suggest it may not be adaptive in terms of supporting a long-term path to health and well-being for youth living in the 21st century. Structural changes that disrupt the systemic factors that increase risk for early puberty (e.g., resource deprivation) as well as supportive relationships can mitigate the risks associated with early puberty, can foster positive outcomes, and may promote adolescents' capability for resilience.
- NEUROBIOLOGICAL DEVELOPMENT
Adolescence is a particularly dynamic period of brain development, second only to infancy in the extent and significance of the neural changes that occur. The nature of these changes—in brain structures, functions, and connectivity—allows for a remarkable amount of developmental plasticity unique to this period of life, making adolescents amenable to change. 4 These normative developments are required to prepare the brain so it can respond to the demands and challenges of adolescence and adulthood, but they may also increase vulnerability for risk behavior and psychopathology ( Paus et al., 2008 ; Rudolph et al., 2017 ). To understand how to take advantage of this versatile adolescent period, it is first important to recognize how and where the dynamic changes in the brain are taking place; Figure 2-2 shows structures and regions of the brain that have been the focus of adolescent developmental neuroscience.
Brain areas important to adolescent development. SOURCE: iStock.com/James Kopp.
In the following sections, we summarize current research on structural and functional brain changes taking place over the course of adolescence. Our summary begins with a focus on morphological changes in gray and white matter, followed by a discussion of structural changes in regions of the brain that have particular relevance for adolescent cognitive and social functioning. We then discuss current theoretical perspectives that attempt to account for the associations between neurobiological, psychological, and behavioral development in adolescence.
Notably, the field of adolescent neuroscience has grown quickly over the past several decades. Advances in technology continue to provide new insights into neurobiological development; however, there is still a lack of agreed-upon best practices, and different approaches (e.g., in equipment, in statistical modeling) can result in different findings ( Vijayakumar et al., 2018 ). Our summary relies on the most recent evidence available and, per the committee's charge, we focus on neurobiological changes that make adolescence a period of unique opportunity for positive development. This is not intended to be an exhaustive review of the literature; moreover, studies tend to use “typically” developing adolescents, which limits our ability to comment on whether or how these processes may change for young people with developmental delays or across a broader spectrum of neurodiversity.
High Plasticity Marks the Window of Opportunity
Studies of adolescent brain development have traditionally focused on two important processes: changes in gray matter and changes in myelin. Gray matter is comprised of neural cell bodies (i.e., the location of each nerve cell's nucleus), dendrites, and all the synapses, which are the connections between neurons. Thus, increases or decreases in gray matter reflect changes in these elements, representing, for instance, the formation or disappearance of synapsis (also known as “synaptogenesis” and “synaptic pruning”). New learning and memories are stored in dynamic synaptic networks that depend equally on synapse elimination and synapse formation. That is, unused connections and cells must be pruned away as the brain matures, specializes, and tailors itself to its environment ( Ismail et al., 2017 ).
White matter, on the other hand, is comprised of myelin. Myelin is the fatty sheath around the long projections, or axons, that neurons use to communicate with other neurons. The fatty myelin insulates the axonal “wire” so that the signal that travels down it can travel up to 100 times faster than it can on unmyelinated axons ( Giedd, 2015 ). With myelination, neurons are also able to recover quickly from firing each signal and are thereby able to increase the frequency of information transmission ( Giedd, 2015 ). Not only that, myelinated neurons can more efficiently integrate information from other input neurons and better coordinate their signaling, firing an outgoing signal only when information from all other incoming neurons is timed correctly ( Giedd, 2015 ). Thus, the increase in white matter is representative of the increase in quality and speed of neuron-to-neuron communication throughout adolescence. This is comparable to upgrading from driving alone on a single-lane dirt road to driving on an eight-lane paved expressway within an organized transportation/transit authority system, since it increases not only the amount of information trafficked throughout the brain but also the brain's computational power by creating more efficient connections.
Recent advances in neuroimaging methods have greatly enhanced our understanding of adolescent brain development over the past three decades. In the mid-2000s developmental neuroscientists described differential changes in gray matter (i.e., neurons) and white matter (i.e., myelin) over the course of adolescence. Specifically, gray-matter volume was believed to follow an inverted-U shape, peaking in different regions at different ages and declining over the course of late adolescence and adulthood ( Lenroot and Giedd, 2006 ). In contrast, cortical white matter, which reflects myelin growth, was shown to increase steadily throughout adolescence and into early adulthood, reflecting increased connectivity among brain regions ( Lenroot and Giedd, 2006 ). The proliferation of neuroimaging studies, particularly longitudinal studies following children over the course of adolescence, has enabled researchers to examine these processes in more detail and across a larger number of participants ( Vijayakumar et al., 2018 ).
Analyses of about 850 brain scans from four samples of participants ranging in age from 7 to 29 years (average = 15.2 years) confirm some previous trends, disconfirm others, and highlight the complexity in patterns of change over time. Researchers found that gray-matter volume was highest in childhood, decreased across early and middle adolescence, and began to stabilize in the early twenties; this pattern held even after accounting for intracranial and whole brain volume ( Mills et al., 2016 ). Additional studies of cortical volume have also documented the highest levels occurring in childhood with decreases from late childhood throughout adolescence; the decrease appears to be due to the thinning of the cortex ( Tamnes et al., 2017 ). Importantly, this finding contrasts with the “inverted-U shape” description of changes in gray-matter volume and disconfirms previous findings of a peak during the onset of puberty ( Mills et al., 2016 ).
For white-matter volume, on the other hand, researchers found that across samples, increases in white-matter volume occurred from childhood through mid-adolescence and showed some stabilizing in late adolescence ( Mills et al., 2016 ). This finding generally confirms patterns observed in other recent studies, with the exception that some researchers have found continued increases in white-matter volume into early adulthood (versus stabilizing in late adolescence; e.g., Aubert-Broche et al., 2013 ). Figure 2-3 shows these recent findings related to gray and white matter.
Cortical gray- and white-matter volume, ages 5 to 30. NOTES: Age in years is measured along the x-axis and brain measure along the y-axis (raw values (mm 3 ). Best fitting models are represented by the solid lines. Dashed lines represent 95-percent confidence (more...)
The widely held belief about a peak in cortical gray matter around puberty followed by declines throughout adolescence was based on the best available evidence at the time. New studies show steady declines in cortical volume beginning in late childhood and continuing through middle adolescence. While the decrease in volume is largely due to cortical thinning rather than changes in surface area, there appear to be complex, regionally specific associations between cortical thickness and surface area that change over the course of adolescence ( Tamnes et al., 2017 ). Discrepant findings can be attributed to a number of factors including head motion during brain imaging procedures (more common among younger participants), different brain imaging equipment, and different approaches to statistical modeling ( Tamnes et al., 2017 ; Vijayakumar et al., 2018 ). There do appear to be converging findings regarding overall directions of change; however, inconsistencies in descriptions of trajectories, peaks, and regional changes will likely continue to emerge as researchers work toward agreed-upon best practices ( Vijayakumar et al., 2018 ). Importantly, though, as Mills and colleagues (2016, p. 279) point out, it is critical to acknowledge that “it is not possible to directly relate developmental changes in morphometric MRI measures to changes in cellular or synaptic anatomy” (also see Mills and Tamnes, 2014 ). In other words, patterns of change in overall gray- or white-matter volume do not provide insight into the specific ways in which neural connections (e.g., synapses, neural networks) may change within the adolescent brain.
In fact, some neural circuity, consisting of networks of synaptic connections, is extremely malleable during adolescence, as connections form and reform in response to a variety of novel experiences and stressors ( Ismail et al., 2017 ; Selemon, 2013 ). Gray-matter reduction in the cortex is associated with white-matter organization, indicating that cortical thinning seen in adulthood may be a result of both increased connectivity of necessary circuitry and pruning of unnecessary synapses ( Vandekar et al., 2015 ). Thus, adolescent brains can modulate the strength and quality of neuronal connections rapidly to allow for flexibility in reasoning and for leaps in cognition ( Giedd, 2015 ).
Structural Changes in the Adolescent Brain
Two key neurodevelopmental processes are most reliably observed during adolescence. First, there is evidence of significant change and maturation in regions of the prefrontal cortex (PFC) involved in executive functioning and cognitive and impulse control capabilities ( Crone and Steinbeis, 2017 ; Steinberg, 2005 ). In other words, areas of the brain that support planning and decision-making develop significantly during the second decade of life. Second, there is evidence of improved connectivity 5 within and between the cortical (i.e., outer) and subcortical (i.e., inner) regions of the brain. Moreover, in both the cortical and subcortical regions, there are age-related and hormone-related changes in neural activity and structure, such as increased volume and connectivity ( Gogtay et al., 2004 ; Østby et al., 2009 ; Peper and Dahl, 2013 ; Wierenga et al., 2014 ).
Over the course of adolescence, regions of the PFC undergo protracted development and significant remodeling. Cortical circuits, especially those that inhibit behavior, continue to develop, enhancing adolescents' capacity for self-regulation ( Caballero and Tseng, 2016 ). Compared to adults, adolescents have a significantly less mature cortical system and tend to utilize these regions less efficiently, and this impacts their top-down cognitive abilities including planning, working memory, impulsivity control, and decision-making ( Casey and Caudle, 2013 ). Ongoing development of structures and connections within the cortical regions corresponds to more efficient balancing of inputs and outputs as adolescents interact with the world.
Changes within subcortical brain regions are also reflected in adolescent capabilities. For instance, increased volume in certain subregions of the hippocampus may predict greater capacity for memory recall and retention in adolescents ( Tamnes et al., 2014 ). Adolescents also display heightened activity in the hippocampus, compared with adults, and differential reward processing in the striatum, which is part of the basal ganglia and plays an important role in motivation and perception of reward. This neural activity may explain their increased sensitivity to rewards and contribute to their greater capacity for learning and habit formation, particularly when incentivized by positive outcomes ( Davidow et al., 2016 ; Sturman and Moghaddam, 2012).
Another subcortical structure, the amygdala, undergoes significant development during puberty and gains new connections to other parts of the brain, such as the striatum and hippocampus ( Scherf et al., 2013 ). The amygdala modulates and integrates emotional responses based on their relevance and impact in context. In conjunction with the amygdala's substantial development, adolescents show higher amygdala activity in response to threat cues 6 than do children or adults ( Fuhrmann et al., 2015 ; Hare et al., 2008 ; Pattwell et al., 2012 ). Consequently, they are prone to impulsive action in response to potential threats 7 ( Dreyfuss et al., 2014 ). Changes in the hippocampus and amygdala may be responsible for suppressing fear responses in certain contexts ( Pattwell et al., 2011 ). Such fearlessness can be adaptive for adolescents as they explore new environments and make important transitions—such as entering college or starting a new job away from home. Children and adults do not tend to show the same kind of fear suppression as adolescents, suggesting that this is unique to this stage of development ( Pattwell et al., 2011 ).
A Neurodevelopmental Perspective on Risk-Taking
In recent years, researchers have worked to reconcile contemporary neuroscience findings with decades of behavioral research on adolescents. There has been a particular emphasis on understanding “risky” behavior through the lens of developmental neuroscience. Risk-taking can be driven by a tendency for sensation-seeking, in which individuals exhibit an increased attraction toward novel and intense sensations and experiences despite their possible risks ( Steinberg, 2008 ; Zuckerman and Kuhlman, 2000 ). This characteristic is heightened during adolescence and is strongly associated with reward sensitivity and drive ( Cservenka et al., 2013 ) as well as the rise in dopamine pathways from the subcortical striatum to the PFC ( Wahlstrom et al., 2010 ). Ironically, as executive function improves, risk-taking based on sensation-seeking also rises, likely due to these strengthened dopamine pathways from the striatum to the PFC regions ( Murty et al., 2016 ; Wahlstrom et al., 2010 ). Despite these stronger sensation-seeking tendencies, however, by mid-adolescence most youth are able to perform cognitive-control tasks at the same level as adults, signaling their capacity for executive self-control ( Crone and Dahl, 2012 ).
Risk-taking can also be driven by impulsivity, which includes the tendency to act without thinking about consequences (impulsive action) or to choose small, immediate rewards over larger, delayed rewards (impulsive choice) ( Romer et al., 2017 ). Impulsive action, which is based on insensitivity to risk, is a form of risk-taking that peaks during early adolescence and is inversely related to working memory ability ( Romer et al., 2011 ). It may also be a consequence of asynchronous limbic-PFC maturation, which is described below. Notably, impulsive actions are seen most frequently in a subgroup of adolescents with pre-existing impairment in self-control and executive function ( Bjork and Pardini, 2015 ). In contrast, impulsive choice behaviors, which are made under conditions of known risks and rewards, do not peak in adolescence. Instead, impulsive choice declines from childhood to adulthood, reflecting the trend of increasing, prefrontal-regulated executive functions throughout adolescence ( van den Bos et al., 2015 ). Interestingly, when given the choice between two risky options with ambiguous reward guarantees, adolescents are more inclined to explore the riskier option than are adults ( Levin and Hart, 2003 ), showing a greater tolerance for ambiguities in reward and stronger exploratory drive ( Tymula et al., 2012 ).
Theoretical models have emerged to explain how neurobiological changes map onto normative “risk” behaviors in adolescence. While some argue that these models and accompanying metaphors may be overly simplistic (e.g., Pfeifer and Allen, 2012 ), the models are nevertheless utilized frequently to guide and interpret research (e.g., Steinberg et al., 2018 ). We briefly discuss two of them here: the “dual systems” model and the “imbalance” model.
The “dual systems” model ( Shulman et al., 2016 ; Steinberg, 2008 ) represents “the product of a developmental asynchrony between an easily aroused reward system, which inclines adolescents toward sensation seeking, and still maturing self-regulatory regions, which limit the young person's ability to resist these inclinations” ( Steinberg et al., 2018 ). The “reward system” references subcortical structures, while the “self-regulatory regions” refer to areas like the PFC. Proponents of the dual-systems model point to recent findings on sensation seeking and self-regulation from a study of more than 5,000 young people spanning ages 10 to 30 across 11 countries. A similar pattern emerged across these settings. In 7 of 11 countries there was a peak in sensation seeking in mid-to-late adolescence (around age 19) followed by a decline. Additionally, there was a steady rise in self-regulation during adolescence; self-regulation peaked in the mid-20s in four countries and continued to rise in five others. The researchers note that there were more similarities than differences across countries and suggest that the findings provide strong support for a dual-systems account of sensation seeking and self-regulation in adolescence.
A second model, the “imbalance” model, shifts the focus away from an orthogonal, dual systems account and instead emphasizes patterns of change in neural circuitry across adolescence. This fine-tuning of circuits is hypothesized to occur in a cascading fashion, beginning within subcortical regions (such as those within the limbic system), then strengthening across regions, and finally occurring within outer areas of the brain like the PFC ( Casey et al., 2016 ). This model corresponds with observed behavioral and emotional regulation—over time, most adolescents become more goal-oriented and purposeful, and less impulsive ( Casey, 2015 ). Proponents of the imbalance model argue that it emphasizes the “dynamic and hierarchical development of brain circuitry to explain changes in behavior throughout adolescence” ( Casey et al., 2016 , p. 129). Moreover, they note that research stemming from this model focuses less on studying specific regions of the brain and more on how information flows within and between neural circuits, as well as how this flow of information shifts over the course of development (e.g., “temporal changes in functional connectivity within and between brain circuits,” p. 129).
Rethinking the “Mismatch” Between the Emotional and Rational Brain Systems
Regardless of whether one of these two models more accurately represents connections between adolescent neurobiological development and behavior, both perspectives converge on the same point: fundamental areas of the brain undergo asynchronous development throughout adolescence. Moreover, adolescent behavior, especially concerning increased risk-taking and still-developing self-control, has been notably attributed to asynchronous development within and between subcortical and cortical regions of the brain. The former drives emotion, and the latter acts as the control center for long-term planning, consideration of outcomes, and level-headed regulation of behavior ( Galván et al., 2006 ; Galván, 2010 ; Mueller et al., 2017 ; Steinbeis and Crone, 2016 ). Thus, if connections within the limbic system develop faster than those within and between the PFC region, 8 the imbalance may favor a tendency toward heightened sensitivity to peer influence, impulsivity, risk-taking behaviors, and emotional volatility ( Casey and Caudle, 2013 ; Giedd, 2015 ; Mills et al., 2014 ).
Indeed, adolescents are more impulsive in response to positive incentives than children or adults, although they can suppress these impulses when large rewards are at stake. Adolescents are also more sensitive than children or adults to the presence of peers and to other environmental cues, and show a heightened limbic response to threats ( Casey, 2015 ). As the cortical regions continue to develop and activity within and across brain regions becomes more synchronized, adolescents gain the capacity to make rational, goal-directed decisions across contexts and conditions.
The idea of asynchrony or “mismatch” between the pace of subcortical development and cortical development implies that these developmental capacities are nonoptimal. Yet, even though they are associated with impulsivity and risk-taking, we should not jump to the conclusion that the gap in maturation between the emotion and control centers of the brain is without developmental benefit. As Casey (2015, p. 310) notes, “At first glance, suggesting that a propensity toward motivational or emotional cues during adolescence is adaptive may seem untenable. However, a heightened activation into action by environmental cues and decreased apparent fear of novel environments during this time may facilitate evolutionarily appropriate exploratory behavior.” While an adolescent's “heart over mind” mentality may compromise judgment and facilitate unhealthy behaviors, it can also spawn creativity and exploration. Novelty seeking can be a boon to adolescents, spurring them to pursue exciting, new directions in life ( Spear, 2013 ).
If properly monitored and cushioned by parents and the community, adolescents can learn from missteps and take advantage of what can be viewed as developmental opportunities . Indeed, because adolescents are more sensitive to rewards and their decision-making ability may skew more toward seeking the positive benefits of a choice and less toward avoiding potential risks, this tendency can enhance learning and drive curiosity ( Davidow et al., 2016 ). To avoid stereotyping all adolescents as “underdeveloped” or “imbalanced,” it is important to recognize the nuances in the different types of risk-taking behavior and to counterbalance a focus on negative outcomes by observing the connections between risk-taking and exploration, curiosity, and other attributes of healthy development ( Romer et al., 2017 ).
The “mismatch” model provides one way of understanding adolescents' capacity for self-control and involvement in risky behavior. A better model of adolescent neurobiological development, some argue, is a “lifespan wisdom model,” prioritizing the significance of experience on brain maturation that can only be gained through exploration ( Romer et al., 2017 ). Indeed, growing evidence shows that adolescents have a distinctive ability for social and emotional processing that allows them to adapt readily to the capricious social contexts of adolescence, and equips them with flexibility in adjusting their motivations and prioritizing new goals ( Crone and Dahl, 2012 ; Nigg and Nagel, 2016 ).
Despite differences between neurobiological models, there is agreement that distinctions between adolescent and adult behaviors necessitate policies and opportunities intended to address adolescent-specific issues. With their heightened neurocognitive capacity for change, adolescents are in a place of both great opportunity and vulnerability. Key interventions during this period may be able to ameliorate the impact of negative experiences earlier in life, providing many adolescents with a pivotal second chance to achieve their full potential and lead meaningful, healthy, and successful lives ( Guyer et al., 2016 ; see also Chapter 3 ).
Cognitive Correlates of Adolescent Brain Development
Reflective of the ongoing changes in the brain described above, most teens become more efficient at processing information, learning, and reasoning over the course of adolescence ( Byrnes, 2003 ; Kuhn, 2006 , 2009 ). The integration of brain regions also facilitates what is called “cognitive control,” the ability to think and plan rather than acting impulsively ( Casey, 2015 ; Casey et al., 2016 ; Steinberg, 2014 ).
Changes in components of cognitive control, such as response selection/inhibition and goal selection/maintenance, along with closely associated constructs such as working memory, increase an individual's capacity for self-regulation of affect and behavior ( Ochsner and Gross, 2005 ). Importantly, each of these aspects of cognitive control appears to have distinct developmental trajectories, and each may be most prominently associated with distinct underlying regions of the cortex ( Crone and Steinbeis, 2017 ). For example, although the greatest developmental improvements in response inhibition and interference control may be observed prior to adolescence, improvements in flexibility, error monitoring, and working memory are more likely to occur throughout the second decade of life ( Crone and Steinbeis, 2017 ). This suggests different developmental trajectories, whereby more basic, stimulus-driven cognitive control processes develop earlier than do more complex cognitive control processes, which rely on internal and abstract representation ( Crone and Steinbeis, 2017 ; Dumontheil et al., 2008 ).
Those functions that do continue to show significant developmental change during adolescence seem to especially rely on the capacity for abstract representation, which is a capacity that has been found to undergo a distinctive increase during adolescence ( Dumontheil, 2014 ). The capacity for abstract representation can relate to both temporal and relational processes, that is, to both long-term goals and to past or future events (temporal) and to representing higher-order relationships between representations (relational) as distinct from simple stimulus features ( Dumontheil, 2014 ). From early through late adolescence (into adulthood), this increase in abstract thinking ability makes teens better at using evidence to draw conclusions, although they still have a tendency to generalize based on personal experience—something even adults do. Adolescents also develop greater capacity for strategic problem-solving, deductive reasoning, and information processing, due in part to their ability to reason about ideas that may be abstract or untrue; however, these skills require scaffolding and opportunities for practice ( Kuhn, 2009 ).
Recent research on cognitive development during adolescence has focused on both cognitive and emotional (or “affective”) processing, particularly to understand how these processes interact with and influence each other in the context of adolescent decision making. First, the capacity for abstract representation and for affective engagement with such representations ( Davey et al., 2008 ) increases the capacity for self-regulation of emotions in order to achieve a goal ( Ochsner and Gross, 2005 ). Indeed, the capacity to regulate a potent, stimulus-driven, short-term response may rely on the ability to mentally represent and affectively engage with a longer-term goal. Furthermore, such stimulus-driven, affective influences on cognitive processing, including on decision making, risk-taking, and judgment, change significantly over the course of adolescence ( Hartley and Somerville, 2015 ; Steinberg, 2005 ).
Beyond individual capacities for cognitive regulation, the social and emotional context for cognitive processing matters a great deal. The presence of peers and the value of performing a task influence how motivating certain contexts may be and the extent to which cognitive processing is recruited ( Johnson et al., 2009 ). Moreover, there is increasing evidence that some of these changes in cognitive and affective processing are linked to the onset of puberty ( Crone and Dahl, 2012 ). Researchers have found that adolescents do better than young adults on learning and memory tasks when the reward systems of the brain are engaged ( Davidow et al., 2016 ).
These changes in cognitive functioning may have adaptive qualities as part of normative adolescent development, even though they also make some individuals more vulnerable to psychopathology, such as depression and anxiety disorders. Notably, the flexibility of the frontal cortical network may be greater in adolescence than in adulthood ( Jolles and Crone, 2012 ). Such flexibility may result in an improved ability to learn to navigate the increasingly complex social challenges that are part of adolescents' social worlds, and as adolescents encounter increasing opportunities for autonomy it may prove to be adaptive. In addition, the ability to shift focus in a highly motivated way could allow more learning, problem solving, and use of creativity ( Kleibeuker et al., 2016 ). Of particular relevance, such emerging abilities may also determine the degree to which an individual can take advantage of new learning opportunities, including mental health–promoting interventions. With the right supports, this capacity for flexibility and adaptability can foster deep learning, complex problem-solving skills, and creativity ( Crone and Dahl, 2012 ; Hauser et al., 2015 ; Kleibeuker et al., 2012 ).
The extensive neurobiological changes in adolescence enable us to reimagine this period as one of remarkable opportunity for growth. Connections within and between brain regions become stronger and more efficient, and unused connections are pruned away. Such developmental plasticity means adolescents' brains are adaptive; they become more specialized in response to environmental demands. The timing and location of the dynamic changes are also important to understand. The onset of puberty, often between ages 10 and 12, brings about changes in the limbic system region resulting in increased sensitivity to both rewards and threats, to novelty, and to peers. In contrast, it takes longer for the cortical regions, implicated in cognitive control and self-regulation, to develop ( Steinberg et al., 2018 ).
Adolescent brains are neither simply “advanced” child brains, nor are they “immature” adult brains—they are specially tailored to meet the needs of this stage of life ( Giedd, 2015 ). Indeed, the temporal discrepancy in the specialization of and connections between cortical and subcortical brain regions makes adolescence unique. The developmental changes heighten sensitivity to reward, willingness to take risks, and the salience of social status, propensities that are necessary for exploring new environments and building nonfamilial relationships. Adolescents must explore and take risks to build the cognitive, social, and emotional skills they will need to be productive adults. Moreover, the unique and dynamic patterns of brain development in adolescence foster flexible problem-solving and learning ( Crone and Dahl, 2012 ). Indeed, adolescence is a seminal period for social and motivational learning ( Fuligni, 2018 ), and this flexibility confers opportunity for adaptability and innovation.
While developmental plasticity in adolescence bears many advantages, as with all aspects of development the environment matters a great deal. The malleable brains of adolescents are not only adaptable to innovation and learning but also vulnerable to toxic experiences, such as resource deprivation, harsh, coercive or antisocial relationships, and exposure to drugs or violence. All of these can “get under the skin” as adolescents develop, or more precisely interact with the brain and body to influence development (see Chapter 3 ).
What is more, the majority of mental illnesses—including psychotic and substance use disorders—begin by age 24 ( Casey, 2015 ; Giedd, 2015 ). This means that we have a collective responsibility to ask, “How can we create the kinds of settings and supports needed to optimize development during this period of life?” This goes well beyond simply keeping youth out of harm's way, and instead signals an urgent need to consider how we design the systems with which adolescents engage most frequently to meet their developmental needs. Notably, scholars studying adolescent developmental neuroscience suggest the next generation of research should consider questions that shift from understanding risk to understanding thriving, and context-specific opportunities to promote it. Such questions for the field include, “How does brain development create unique opportunities for learning and problem solving?,” “Is the adolescent brain more sensitive to some features of the social environment than others?,” and “Are trajectories of change [in cognitive control and emotional processing] steeper or quicker during some periods than others, potentially providing key windows for input and intervention?” ( Fuligni et al., 2018 , p. 151).
- PSYCHOSOCIAL DEVELOPMENT IN ADOLESCENCE
As described above, young people develop increased cognitive abilities throughout adolescence. These cognitive abilities provide the capacity for other aspects of psychosocial development that occur during the period. This section describes the psychosocial developmental tasks—including developing identity and a capacity for self-direction—that adolescents complete during their transition to adulthood. Understanding one's self, understanding one's place in the world, and understanding one's capacity to affect the world (i.e., agency) are all processes that begin to take shape during adolescence in tandem with the physiological, neurobiological, and cognitive changes discussed above.
The trajectory of social and emotional development in adolescence may perhaps be best characterized as a time of increasing complexity and integration. As is true of their neurobiological development during the period, adolescents' capacity for understanding and engaging with self, others, and societal institutions requires both integration and deepening. It requires adolescents to integrate multiple perspectives and experiences across contexts, and also to deepen their ability to make sense of complex and abstract phenomena.
This section begins with a summary of developmental trends in adolescent self- and identity development at a broad level, followed by a brief discussion of how these trends reflect recent findings from developmental neuroscience. From there, we discuss group-specific social identities. While there are many critical dimensions of social identity (e.g., gender, social class, religion, immigration status, disability, and others), we use race and sexuality as exemplars given the recent, monumental shifts in racial/ethnic demographics and in the social and political climate around sexual minority status in the United States. The focus on race and sexuality is not intended to minimize other dimensions of identity; indeed, identity development is a salient process for all adolescents regardless of social group memberships. Moreover, as we discuss below, developmental scientists are increasingly calling for research that examines the intersectional nature of identities, both at the individual level as well as in ways that reflect membership in multiple groups that have historically experienced marginalization ( Santos and Toomey, 2018 ).
Finding an answer to the question, “Who am I?” is often viewed as a central task of adolescence. Decades ago, Erik Erikson (1968) argued that during adolescence, youth take on the challenge of developing a coherent, integrated, and stable sense of themselves, and that failing to do so may make the transition to adult roles and responsibilities more difficult. Erikson's concept of identity development assumes opportunities for exploration and choice and may or may not generalize across global contexts ( Arnett, 2015 ; Syed, 2017 ). However, it has utility in the United States, where societal structures and dominant values such as independence and individuality encourage identity exploration.
Closely related to the question, “Who am I?” is the question, “ How do I see myself?” ( Harter, 2012 ). McAdams (2013) describes the developmental trajectory of “self” using a set of sequential metaphors: the “social actor” in childhood (because children engage in action) grows to become a “motivated agent” in adolescence (because teens are more purposeful and agent-driven, guided by values, motives, and hopes), and finally an “autobiographical author” in emerging adulthood, a time when young people work on building a coherent self-narrative. Studies of youth across the span of adolescence show that, for many young people, the sense of self and identity become more integrated, coherent, and stable over time ( Harter, 2012 ; Klimstra et al., 2010 ; Meeus et al., 2010 ). Importantly, theory suggests and empirical evidence supports the idea that having a more “achieved” identity and integrated sense of self relates to positive well-being in adulthood and even throughout the life course (e.g., Kroger and Marcia, 2011 ; Meca et al., 2015 ; Schwartz et al., 2011 ).
While there is great variability across youth, there are also some distinct developmental trends in the emergence of self and identity. In early adolescence, young teens' self-definitions are increasingly differentiated relative to childhood. They see themselves in multiple ways across various social and relational contexts, for example one way when with their family and another way when with close friends in the classroom. Although a young adolescent may carry a great number of “abstractions” about his or her self, these labels tend to be fragmented and sometimes even contradictory ( Harter, 2012 ). For instance, a 13-year-old may view herself as shy and quiet in the classroom, as loud and bubbly with close friends, and as bossy and controlling with her younger siblings. Longitudinal studies suggest that some perceptions of self (e.g., academic self-concept) decline in early adolescence as youth transition to middle school; however, there is a great deal of individual variability, variability across domains (e.g., academic vs. behavioral self-concept), and variability by gender (higher athletic self-concept among males vs. females; Cole et al., 2001 ; Gentile et al., 2009 ).
In middle adolescence, teens may still hold onto multiple and disjointed abstractions of themselves; however, their growing cognitive abilities allow for more frequent comparisons among the inconsistencies, and heightened awareness of these contradictions can create some stress ( Brummelman and Thomaes, 2017 ; Harter, 2012 ). In this period, youth may also be more aware that their conflicting self-characterizations tend to occur most often across different relationship contexts. As in early adolescence, discrepancies between real and ideal selves can create stress for some youth, but as teens develop deeper meta-cognitive and self-reflection skills, they are better able to manage the discrepancies. To continue with the same hypothetical teen introduced above at age 13, at age 16 she might view being shy and quiet in the classroom and loud and bubbly with friends as parts of a more holistic, less fragmented sense of self.
Older adolescents have greater abilities to make sense of their multiple abstractions about self. They can reconcile what seem like contradictory behaviors by understanding them in context ( Harter, 2012 ). For instance, older teens are more likely to view their different patterns of behavior across settings as reflecting a positive trait like “flexibility,” or they may characterize themselves as “moody” if they vacillate between positive and negative emotions in different situations. While peers are still important in late adolescence, youth may rely on them less when making self-evaluations; they also have greater capacity for perspective-taking and attunement to others, especially in the context of supportive relationships.
Emerging adulthood provides additional opportunities for experimenting with vocational options, forming new friendships and romantic relationships, and exercising more independent decision-making ( Arnett, 2015 ; Harter, 2012 ; Schwartz et al., 2005 ). Many young adults shift from “grand” visions of possible selves to visions that are narrower and directly related to immediate opportunities. New experiences across contexts—like attending college or transitioning into the workforce—can shape whether emerging adults develop an authentic and integrated sense of self.
With the normative development of heightened sensitivity to social information, some youth may rely heavily on peer feedback in self-evaluation; however, parents still play an important role in supporting a positive sense of self, especially when they are attuned to youths' needs and couple their high expectations with support ( Harter, 2012 ). Indeed, secure and supportive relationships with parents can help early and middle adolescents develop a clear sense of self ( Becht et al., 2017 ) and can buffer youth who are socially anxious against harsh self-criticism ( Peter and Gazelle, 2017 ).
Identity and Self: A Neurobiological Perspective
Recent advances in developmental neuroscience appear to complement decades of behavioral research on youth. For instance, the integrated-circuitry model of adolescent brain development discussed in the previous section ( Casey et al., 2016 ), along with other models emphasizing the growing integration within and between emotionally sensitive brain regions (e.g., the limbic system) and those involved in planning and decision making (e.g., the cortical regions), correspond with the observation that adolescents develop a more coherent sense of self over time and experience. Likewise, changes observed in social and affective regions of the brain during adolescence align with behavioral tendencies toward exploration and trying new things ( Crone and Dahl, 2012 ; Flannery et al., 2018 ). Although the evidence base is still growing, recent studies document how self-evaluation and relational identity processes are linked with regions of the brain like the ventromedial PFC (vmPFC) (which plays a role in the inhibition of emotional responses, in decision making, and in self-control) and the rostral/perigenual anterior cingulate cortex (which plays a role in error and conflict detection processes). In particular, activity in these regions increases from childhood through adolescence in a manner consistent with changes in identity development ( Pfeifer and Berkman, 2018 ).
Recent theoretical models of value-based decision making suggest specific ways in which identity development and neural development are linked in adolescence ( Berkman et al., 2017 ; Pfeifer and Berkman, 2018 ). An important premise is that while adolescents may be more sensitive to social stimuli such as peer norms and to rewarding outcomes such as tangible gains, their sense of self is still a critical factor influencing their behavior. In other words, while social norms and tangible gains and costs represent some of the “value inputs,” their construal of self and identity are also factors in their decision making. Moreover, neural evidence, like the activation observed in the vmPFC during self- and relational identity tasks, suggests that identity and self-related processes may play a greater role in value-based decision making during adolescence than they do in childhood ( Pfeifer and Berkman, 2018 ).
Social Identities in Adolescence
As many youth work toward building a cohesive, integrated answer to the question, “Who am I?,” the answer itself is shaped by membership across multiple social identity groups: race, ethnicity, nationality, sexuality, gender, religion, political affiliation, ability status, and more. Indeed, in the context of increasingly complex cognitive abilities and social demands, youth may be more likely to contest, negotiate, elaborate upon, and internalize the meaning of membership in racial/ethnic, gender, sexual, and other social identity groups (e.g., Umaña-Taylor et al., 2014 ). From a developmental perspective, these tasks are paramount in a pluralistic, multiethnic and multicultural society like the United States, which, as discussed in Chapter 1 , is more diverse now than in previous generations.
Ethnic-Racial Identity. Currently, our nation's population of adolescents is continuing to increase in diversity, with no single racial or ethnic group in the majority. A burgeoning area of study over the past two decades concerns ethnic-racial identity (ERI), and research in this field has found that for most youth, particularly adolescents of color, ERI exploration, centrality, and group pride are positively related to psychosocial, academic, and even health outcomes ( Rivas-Drake et al., 2014 ). ERI is multidimensional—it includes youths' beliefs about their group and how their race or ethnicity relate to their self-definition—both of which may change over time ( Umaña-Taylor et al., 2014 ). For immigrant youth, developing their own ERI may involve an internal negotiation between their culture of origin and that of their new host country, and most immigrant youth show a great deal of flexibility in redefining their new identity ( Fuligni and Tsai, 2015 ). Regardless of country of origin, making sense of one's ERI is a normative developmental process that often begins in adolescence ( Williams et al., 2012 ). Indeed, given that research has consistently found ERI to be associated with adaptive outcomes, dimensions of ERI can be understood as components of positive youth development ( Williams et al., 2014 ).
Sexual Orientation and Gender Identity. One of the distinctive aspects of adolescence is the emergence and awareness of sexuality, and a related aspect is the emerging salience of gender roles and expression. Adolescence is also a time when identities or sense of self related to gender and sexuality are developed and solidified ( Tolman, 2011 ), and this occurs in a period during which sexuality and gender norms are learned and regulated by peers ( Galambos et al., 1990 ). In this developmental context, LGBTQ youth begin to understand their sexual and gender identities.
The growing societal acceptance and legal recognition of LGBTQ youth is implicated in the recent observed drop in the age at which most of these young people “come out,” that is, disclose their same-sex sexual identities. Less than a generation ago, LGBTQ people in the United States typically came out as young adults in their 20s; today the average age at coming out appears to be around 14, according to several independent studies ( Russell and Fish, 2017 ).
In the context of such changes and growing acceptance and support for LGBTQ youth developing their sexual identity, it might be expected that the longstanding health and behavior disparities between these adolescents and heterosexual and cis-gender adolescents would be lessening. Yet multiple recent studies challenge that conclusion. Things do not appear to be getting “better” for LGBTQ youth: rather than diminishing, health disparities across multiple domains appear to be stable if not widening ( Russell and Fish, 2017 ). This pattern may be explained by several factors, including greater visibility and associated stigma and victimization for LGBTQ youth, just at the developmental period during which youth engage in more peer regulation and bullying in general, especially regarding sexuality and gender ( Poteat and Russell, 2013 ). In fact, a meta-analysis of studies of homophobic bullying in schools showed higher levels of homophobic bullying in more recent studies ( Toomey and Russell, 2016 ). These patterns point to the importance of policies and programs that help schools, communities, and families understand and support LGBTQ (and all) youth (see Chapter 7 ).
Identity Complexity. Beyond race, gender, or sexuality alone, having a strong connection to some dimension of social identity—which could also be cultural, religious, or national—appears to be important for psychological well-being in adolescence ( Kiang et al., 2008 ). Recent research also suggests that young adolescents benefit from having a more complex, multifaceted identity that goes beyond stereotypical expectations of social-group norms, especially when it comes to inclusive beliefs ( Knifsend and Juvonen, 2013 ). For instance, a youth who identifies as a Black, 13-year-old, transgender female who plays volleyball and loves gaming is apt to have more positive attitudes toward other racial/ethnic groups than she would if she viewed racial/ethnic identity and other social identities as necessarily convergent (such as the notion that “playing volleyball and being a gamer are activities restricted to youth from specific racial/ethnic groups”; Knifsend and Juvonen, 2014 ).
However, context is still important, and the association between identity complexity and inclusive beliefs in early adolescence tends to be stronger for youth who have a diverse group of friends ( Knifsend and Juvonen, 2014 ). Among college-age students there is also variation by race and ethnicity. For instance, the positive association between having a complex social identity and holding more inclusive attitudes toward others has been found most consistently among students who are members of the racial/ethnic majority; for members of racial/ethnic minority groups, convergence between racial/ethnic identity and other in-group identities is not related to attitudes toward other racial/ethnic groups ( Brewer et al., 2013 ). Beyond outgroup attitudes, there is evidence that social identity complexity has implications for youths' own perceptions of belonging; for instance, Muslim immigrant adolescents (ages 15 to 18) with greater identity complexity reported a stronger sense of identification with their host country ( Verkuyten and Martinovic, 2012 ).
Social Identity and Neurobiology
Cultural neuroscience provides some insight into how social identity development may manifest at the neurobiological level, although there is still much work to be done to understand the deep associations between biology and culture ( Mrazek et al., 2015 ). In adolescence, evidence suggests, areas of the brain attuned to social information may be undergoing shifts that heighten youths' social sensitivity ( Blakemore and Mills, 2014 ), and of course, adolescents' “social brains” develop in a cultural context. For instance, we know the amygdala responds to stimuli with heightened emotional significance; in the United States, where negative stereotypes about Blacks contribute to implicit biases and fears about them, amygdala sensitivity to Black faces has been documented in adult samples ( Cunningham et al., 2004 ; Lieberman et al., 2005 ; Phelps et al., 2000 ).
In a study of children and adolescents (ages 4 to 16) in the United States, Telzer and colleagues (2013) found that amygdala activation in response to racial stimuli, such as images of Black faces, was greater in adolescence than during childhood. They suggest that identity processes reflecting heightened sensitivity to race, along with biological changes (e.g., those stemming from puberty) related to a “social reorientation” of the amygdala, may be among the mechanisms that explain these race-sensitive patterns of activation in adolescence ( Telzer et al., 2013 ). Importantly, neural activation appears to vary based on the context of social experiences. Specifically, the amygdala activation observed in response to Black faces was attenuated for youth who had more friends and schoolmates of a race differing from their own (i.e., cross-race friends).
The foregoing findings converge with psychobehavioral studies that demonstrate the importance of school and friendship diversity. Attending diverse middle schools and having more cross-race friends is associated with more positive attitudes toward outsider groups, less social vulnerability, greater social and academic competence, and better mental health ( Graham, 2018 ; Williams and Hamm, 2017 ). Adolescence is a period of transformation in social cognition ( Blakemore and Mills, 2014 ; Giedd, 2015 ), so in light of the findings from psychobehavioral and cultural neuroscience research on the benefits of diversity, important questions may be asked about whether adolescence is a critical period for providing exposure to difference. For instance, should we expect the benefits of exposure to diversity to be maximized if such exposure occurs during adolescence, or are benefits most likely with cumulative exposure that begins well before this period? 9
Identity Development in Context
Identity development takes place in specific socio-cultural, political, and historical contexts. As an example, consider recent cultural and political shifts regarding same-sex relationships in the United States: in the period of one generation there has been dramatic social change regarding understanding and awareness of LGBTQ lives and issues. For context, consider that less than 20 years ago, marriage between same-sex couples was just beginning to be recognized anywhere in the world (the first country to do so was the Netherlands in 2001); less than 20 years later, 25 countries have legalized same-sex marriage, and recent surveys show that most young people in the United States approve of same-sex marriages ( Pew Research Center, 2015 ). Moreover, the identity language and labels used among youth who are often placed under the umbrella of LGBTQ have continued to rapidly evolve. A growing number of LGBTQ youth say they have a nonbinary gender identity (i.e., neither male nor female) or sexual identity (e.g., pansexual, bisexual, queer) ( Hammack, 2018 ). Indeed, young people appear to be leading a movement toward challenging existing categories and constructing new identities.
Meanwhile, in the past decade there has been a dramatic change in public awareness and understanding of transgender identities. Popular attention to the gender changes of a number of celebrities coincided with growing emergence and awareness of transgender children. 10 Thus, a subject that was literally unknown by most people in the United States has within a decade become the subject of public discussion and political debate. School systems are grappling with gender change and accommodations for transgender students, and the typical developmental challenges of adolescence are being navigated by a growing number of openly transgender, gender-nonbinary, or gender-nonconforming adolescents ( Wilson et al, 2017 ).
Developmental scientists have recently called for a deeper investigation of the ways in which intersecting axes of oppression shape youth development, often referred to as “intersectionality” ( Crenshaw, 1990 ; Santos and Toomey, 2018 ; Velez and Spencer, 2018 ). Indeed, against a backdrop of social stratification and oppression, relationships between identity, experience, and behavior may not operate the same way for all youth ( Spencer, 1995 ). For example, the way in which knowledge is socially constructed contributes to maintaining systems and structures that control and exclude marginalized populations such as people with disabilities ( Peña et al., 2016 ). Smart and Smart (2007) argue that society has historically viewed people with disabilities from a medical perspective, in which individuals were labeled as ill, dysfunctional, and in need of medical treatment. This approach perpetuates an ableist worldview that suggests people with disabilities should strive toward an able-bodied norm, reflecting society's perceptions that certain abilities are essential to fully function in the world ( Hutcheon and Wolbring, 2012 ). This example highlights why an intersectional perspective is important for understanding adolescent psychosocial development in context, both for considering systemic factors that shape opportunities and for broadening the range of questions, values, samples, and experiences that have been defined and studied from a dominant-group perspective ( Syed et al., 2018 ). Ultimately, intersectional approaches and related integrative models are needed to understand how youth development in context can lead to further marginalization for some youth ( Causadias and Umaña-Taylor, 2018 ) or to adaptability and resilience for others ( Gaylord-Harden et al., 2018 ; Suárez-Orozco et al., 2018 ).
We have long considered identity exploration as a hallmark of adolescence. An adolescent's identity is an emerging reflection of his or her values, beliefs, and aspirations, and it can be constructed and reconstructed over time and experience. Multiple factors—family, culture, peers, media—shape identity development, but young people are also active agents in the process. Movement toward stability and coherence is normative, yet there remain dynamic elements that shape the relationship between identity and behavior; teens often select activities that feel identity-congruent, and may interpret and respond to a given situation based on aspects of identity that are salient in the moment ( Oyserman, 2015 ; Oyserman and Destin, 2010 ). This has implications for adolescents' experiences in important contexts such as school. Identity processes are connected to a larger set of self-development characteristics, including self-regulation, self-efficacy, and a sense of agency, all of which youth need to help develop and commit to meaningful goals. Ensuring that adolescents understand how all identities can be consistent with their current academic choices and future educational and vocational aspirations is an important consideration for the education system and is discussed further in Chapter 6 .
Recent neuroscientific findings suggest that changes in social and affective regions of the brain correspond to developmental changes in identity development. Moreover, identity and self-related processes may play a greater role in decision making during adolescence than they do in childhood. Youth may also experience identity congruence, affirmation, or marginalization through their interpersonal interactions with policies, sociopolitical events, and historical factors. Ultimately, how adolescents' multifaceted identities are manifested—neurobiologically, behaviorally, and otherwise—and the role identity plays in their overall well-being depend a great deal on experiences in context. This requires us to reflect on the nature of the contexts in which adolescents are developing their identities.
Consider, for example, that a youth's likelihood of involvement in extremist organizations may be heightened as they search for meaningful in-groups, if they accept group beliefs without questioning them (i.e., identity foreclosure), and/or if they feel their personal or group identities are under threat ( Dean, 2017 ; Schwartz et al., 2009 ). As Schwartz and colleagues note, “providing mainstream paths for young people, within the cultural constraints of their society, can help to alleviate the anger, frustration, and hopelessness leading many young people [towards extremism]” ( Schwartz et al., 2009 , p. 553). While the overwhelming majority of adolescents do not become involved in extremist groups, acknowledging this possibility underscores how the significant opportunities afforded by identity exploration in adolescence can be thwarted by conditions that increase the likelihood of marginalization.
Adolescent Capacity for Self-Direction
As adolescents ask, “Who am I?” their growing cognitive capacities also permit reflection on themselves in relation to a broader collective: “What is my role in my school? my community? my society?” As adolescents grow older, they have more opportunities to make their own choices in domains that matter for future outcomes, and their capacity to make such choices also increases; Box 2-1 describes youths' perspectives on this emerging autonomy, agency, and independence.
Youth Perspectives: Sense of Agency, Purpose, and Autonomy.
In the following section, we discuss developmental changes in autonomy, purpose, and agency in adolescence. One might think of these three things not only as competencies that develop within adolescents, but also as resources or opportunities they need to thrive as they transition into adult roles. Framing them as both capacities of the individual youth and as characteristics afforded by supportive settings reminds us that developmental pathways that lead to thriving in adulthood are not forged by adolescents alone, but instead require alignment between youths' strengths and the resources available in their environments.
Striving for Autonomy While Remaining Connected
For most adolescents, establishing a level of independence and self-sufficiency is normative. This typically involves individuating from one's family. However, gaining a sense of autonomy does not mean that adolescents strive to become detached from their family. Indeed, the developmental task for most teens is about establishing a balance between autonomy and connection ( McElhaney et al., 2009 ). While many adolescents would like more autonomy for making decisions, this varies by age and domain ( Daddis, 2011 ; Smetana, 2011 ). Most youth report having enough autonomy when it comes to making moral decisions, but younger adolescents tend to desire more autonomy for personal matters (e.g., hairstyle and clothing choices) and conventional matters (e.g., cursing/swearing) than older teens. This increase in desired autonomy among younger teens maps onto findings that older teens report having more autonomy across multiple domains than their younger peers.
Not only do young adolescents have less autonomy than older youth, they also tend to overestimate how much autonomy their peers have; in other words, younger adolescents tend to think their friends are allowed to have more control over their choices and behaviors than they actually do. Adolescents who think they have low levels of autonomy over decisions also tend to believe their friends have more autonomy, whereas adolescents who feel they have enough autonomy are less influenced by perceptions of their peers ( Daddis, 2011 ).
Autonomy and Culture
The concept of “autonomy” implies independence, which generally is accepted as a core value among cultures oriented toward individualism. In contrast, one might expect youth from cultures oriented toward collectivism and interdependence to be more inclined toward harmonious, less conflictual relationships with parents and a lower desire for individuation. However, evidence suggests that teens in many cultures, both those labeled “individualist” and those labeled “collectivist,” strive to develop autonomy, and levels of parent-teen conflict are similar in immigrant and nonimmigrant families ( Fuligni and Tsai, 2015 ; Tsai et al., 2012 ). Studies of youth from multiple ethnic backgrounds in the United States, including those who are U.S.-born and those from immigrant families, show that most adolescents express a desire to have control over personal choices ( Phinney et al., 2005 ). Importantly, while youth across cultural backgrounds identify autonomy as important, there can be culturally relevant variations in how autonomy is defined. For example, some adolescents from Asian American heritage groups describe autonomy through the lens of “interdependence” ( Russell et al., 2010 ).
Examining Autonomy and Culture “Under the Skin”
While all teens may desire autonomy from their parents and seek identities and self-definitions that go beyond their role in the family, adolescents in immigrant families in the United States may have a stronger sense of family obligation relative to youth in nonimmigrant families. Recent findings from the field of cultural neuroscience demonstrate the integration between biology and sociocultural context ( Telzer et al., 2010 ; Fuligni and Telzer, 2013 ). In one study, White and Latinx older adolescents participated in laboratory-based tasks in which they were asked to allot cash rewards to themselves or to their families; during the task their patterns of brain activity were observed using functional magnetic resonance imaging (fMRI). While youth from both groups allotted cash rewards to family at the same rate, among Latinx youth the “reward centers” of the brain were more activated when they contributed to family, whereas White youth showed more brain activity in the reward centers when allotting cash to themselves. Across both groups, those who felt a stronger sense of family identification and who felt fulfilled by contributing to family had more activation in the reward centers of the brain when allotting cash to their family. Thus, the cultural meaning that youth and families make around issues of autonomy, connection, and obligation are connected to neurobiological responses in the context of family contribution.
Some studies show linkages between broad cultural orientations, such as being more individually or more collectively oriented, and patterns of neural response ( Mrazek et al., 2015 ). Moreover, cultural neuroscientists posit that developmental growth and transitions in neural activity shape the transmission of cultural values, like preference for social hierarchy ( Mrazek et al., 2015 ). In addition to the vmPFC and the anterior cingulate cortex regions of the brain implicated in personal identity development, researchers speculate that the temporoparietal junction may be implicated in culturally embedded identities that orient youth toward independence or interdependence ( Cheon et al., 2011 ; Mrazek et al., 2015 ; Saxe et al., 2009 ).
Finding Meaning and Taking Action: Purpose and Agency
Purpose has been defined as “a stable and generalized intention to accomplish something that is at once meaningful to the self and of consequence to the world beyond the self” ( Damon et al., 2003 , p. 121) and also as “a central, self-organizing life aim that organizes and stimulates goals, manages behaviors, and provides a sense of meaning” ( McKnight and Kashdan, 2009 , p. 242). Thus, one's sense of purpose can be oriented toward life aims that are self-focused or toward aims that transcend the self ( Sumner et al., 2018 ; Yeager et al., 2012 ). Higher scores on measures of purpose are generally associated with more positive psychological wellbeing, a more consolidated identity, a deeper sense of meaning, and fewer health-compromising behaviors; a sense of purpose is also positively correlated with religiosity and spirituality ( Burrow and Hill, 2011 ; Sumner et al., 2018 ). Moreover, there is evidence that purpose helps explain associations between identity commitment and positive youth adjustment ( Burrow and Hill, 2011 ).
For all adolescents, developing a sense of purpose requires some support, particularly while their sense of orientation toward the future is still under development ( Steinberg et al., 2009 ). For adolescents who experience marginalization—by virtue of membership in one or more groups that experience systemic oppression ( García Coll et al., 1996 ; Causadias and Umaña-Taylor, 2018 )—developing a sense of purpose may be compromised if structural discrimination makes links between present action and future outcomes unpredictable (e.g., for adolescents with an undocumented immigration status) ( Gonzales, 2016 ; Sumner et al., 2018 ). Adolescents experiencing marginalization may internalize such messages as they become more aware of their own external realities; the messages may also be reinforced through family socialization practices. For example, researchers studying low-income White adolescents suggest that parents' messages of “isolation and threat, helplessness and hopelessness, and live fast, die young,” which may be adaptive in the short-term and in the immediate settings where the families live, can compromise youth's sense of purpose, hope, and agency ( Jones et al., 2018 ).
Agency to Take Action
Adolescents' growing competencies in flexible problem-solving, their awareness of and concern with others, and their openness to exploration and novelty ( Crone and Dahl, 2012 ) make adolescence a particularly opportune time to allow for agency and leadership ( Flanagan and Christens, 2011 ). Indeed, young people have been at the helm of social movements for centuries. For some youth, active civic engagement may be an adaptive means for coping with systemic injustice, particularly for those in historically marginalized communities ( Diemer and Rapa, 2016 ; Ginwright et al., 2006 ; Hope and Spencer, 2017 ). In a recent multi-methods study of middle and late adolescents in seven community organizations (four in the United States, two in Ireland, and one in South Africa), many of which served low-income or working class communities, researchers documented multiple benefits of civic engagement. Findings suggest the context of youth organizing promoted the skills of critical thinking and analysis, social and emotional learning, and involvement in community leadership and action ( Watts, 2018 ; Watts et al., 2011 ).
In relation to research on community leadership and action, recent work has examined the construct of “critical consciousness” among adolescents ( Watts et al., 2011 ). Contemporary definitions of critical consciousness, grounded in the work of Brazilian educator Paolo Freire (1970) , include the elements of critical reflection, motivation, and action ( Diemer et al., 2015 ). These core concepts have informed the development of new measures of critical consciousness for middle and late adolescents (e.g., Diemer et al., 2017 ; McWhirter and McWhirter, 2016 ; Thomas et al., 2014 ). Youth with higher levels of critical consciousness are more likely to recognize injustice and may feel a greater sense of agency or efficacy in responding to it ( Diemer and Rapa, 2016 ; Shedd, 2015 ). Critical consciousness is also positively associated with vocational and educational attainment ( Diemer et al., 2010 ; Luginbuhl et al., 2016 ; McWhirter and McWhirter, 2016 ).
Capacity for Self-Direction as a Developmental Opportunity
While there is general agreement about the benefits of purpose and agency in adolescence, ongoing work is needed to better understand the circumstances under which they are best fostered and the way they relate to other processes (e.g., critical consciousness) and to behavior (e.g., volunteering, social activism). For instance, do opportunities for critical reflection contribute to an adolescent's sense of purpose? Are community service or civic action necessary for building an adolescents' belief in their own agency to create change?
Additional research might determine whether a sense of purpose that transcends the self has greater positive impact on an adolescent than one that is more self-focused. Current work in this area suggests that a self-transcendent sense of purpose better predicts academic regulation, performance, and persistence among high school students ( Yeager et al., 2014 ); however, whether this extends beyond the school context is unclear. As research methods and methods in studies of critical consciousness continue to advance (e.g., Diemer et al., 2015 ), we may have a better understanding of how this particular kind of agency develops across adolescence, and for whom and under what conditions greater critical consciousness is most beneficial. Finally, an emerging body of work on adolescents' contribution mindset (i.e., giving to others; Fuligni and Telzer, 2013 ) and value-based decision making ( Pfeifer and Berkman, 2018 ) may provide some insight into the neurobiological correlates underlying the cognitive and social skills needed for developing purpose.
Over the course of adolescence, youth gain the cognitive skills needed to reflect on complex questions about their aims in life and their role in the world. They can question the legitimacy and fairness of everyday experiences and of social institutions. Indeed, the social systems they must navigate—schools, employment, health care, justice—are quite complex and often require them to engage in independent decision making. Two important questions stemming from this reality are, “What experiences are needed to support adolescents' agency as they transition into adult roles?” and “What might our society look like if all adolescents felt a sense of commitment to something personally meaningful and goal-directed that extends beyond the self?” ( Bronk, 2014 ).
Supporting opportunities for autonomy and agency and fostering a sense of purpose may help adolescents explore meaningful questions about who they are, and about their place in the world and their capacity to shape it. Continuing shifts in the social, cultural, economic, and technological contexts in which today's adolescents are developing require thoughtful consideration as to how, when, and where adolescents can find and act upon ideas and issues they find meaningful. For example, religion has traditionally been a context where youth have found purpose and meaning, and religious involvement is associated with civic engagement ( Furrow et al., 2004 ; Pew Research Center, 2019 ; Sumner et al., 2018 ). Religion can also be protective against stressors like discrimination and against negative mental health outcomes ( Hope et al., 2017 ). However, adolescents and young adults today are less likely to be religiously engaged than those in earlier generations ( Pew Research Center, 2018 ). If faith-based institutions are playing a less central role in the lives of greater numbers of today's adolescents, this brings to the fore questions about the alternative settings and experiences to which youth are turning and whether these settings play a comparable role in fostering involvement and purpose.
Although there is great variation in how the skills of autonomy, purpose, and agency manifest and how they are defined and valued, adolescents should be afforded opportunities—in families, schools, or out-of-school settings—to develop them. Such skills not only are important to support the transition to adulthood, but also make adolescence itself a period that fosters a propensity to choose their own paths in life and to shape the roles they want to play in their communities ( Fuligni, 2018 ).
Adolescence, spanning the period from the onset of puberty to adulthood, is a formative period where changes in cognition, affect, and interpersonal behavior occur alongside the most extensive biological transitions since infancy, especially with respect to pubertal and brain development. Collectively, the pubertal, neurobiological, cognitive, and psychosocial changes occurring during adolescence mark this as a period of great opportunity for adolescents to flourish and thrive.
While often thought of as a time of turmoil and risk for young people, adolescence is more accurately viewed as a developmental period rich with opportunity for youth to learn and grow. If provided with the proper supports and protection, normal processes of growth and maturation can lead youth to form healthy relationships with their peers and families, develop a sense of identity and self, and experience enriching and memorable engagements with the world. Adolescence thus forms a critical bridge between childhood and adulthood and is a critical window of opportunity for positive, life-altering development. As a positive window of opportunity, adolescence marks a period of optimism, where the assets of youth and their development may be capitalized for the betterment of society.
Important questions emerge from these findings. What are the “windows of opportunity” for promoting a positive developmental trajectory and adaptive plasticity? What are the mechanisms that shape developmental trajectories, for better or worse, during adolescence and over the life course? To begin to answer these, in the next chapter we consider the emerging science of epigenetics as it reveals the ongoing plasticity of the brain and the reciprocal influences of brain on body and vice versa.
The average child in the United States experiences the onset of puberty between the age of 8 and 10 years.
HPG hormones can bind within cell nuclei and change the transcription and expression of genes to regulate further hormone production, brain function, and behavior ( Melmed et al., 2012 ; Sisk and Foster, 2004 ). The process begins in the brain when a gonadotropin-releasing hormone (GnRH) is secreted from the hypothalamus. The activation of GnRH is not unique to the pubertal transition; GnRH is also active during pre- and perinatal periods of development but undergoes a quiescent period during the first year of postnatal life until it reawakens during the pubertal transition. GnRH stimulates the pituitary gland to secrete luteinizing hormone (LH) and follicle-stimulating hormones (FSH), which then stimulate the ovary and testes to secrete estradiol and testosterone.
For more information on the National Longitudinal Study of Adolescent Health, see https://www .cpc.unc.edu /projects/addhealth .
See Chapter 3 for a discussion of the adaptive plasticity of adolescence and the potential of interventions during adolescence to mediate deficiencies from earlier life periods.
“Connectivity” refers to the formation of synapses, or connections between neurons; groups of interconnected neurons form circuit-like neural networks.
The threat cues used in the research cited here were pictures of “fearful faces,” which serve as a social cue of impending danger.
Impulsive action in response to potential threat was assessed using a “go/no-go” task. Simply put, this is a task in which participants are presented with two types out of three facial emotions (“happy” or “calm” or “fearful”) that are randomly assigned as “go” (stimulate action = press a button) or “no-go” (inhibit action = do not press button).
While there may be asynchronous development of circuits within specific regions of the brain during adolescence, this does not mean that these regions are “fixed” by the end of adolescence; instead, people retain the ability for neural plasticity and change throughout the life course (see Chapter 3 ).
For instance, rodent models suggest that empathy is shaped by social context (e.g., rats usually assist members of their own genetic strain, but will extend their prosocial behavior to unrelated peers if they are raised together; Bartal et al., 2011 ; Meyza et al., 2017 ).
See, for example, “Beyond ‘He' or ‘She': The Changing Meaning of Gender and Sexuality,” TIME Magazine, March 16, 2017.
- Cite this Page National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Division of Behavioral and Social Sciences and Education; Board on Children, Youth, and Families; Committee on the Neurobiological and Socio-behavioral Science of Adolescent Development and Its Applications; Backes EP, Bonnie RJ, editors. The Promise of Adolescence: Realizing Opportunity for All Youth. Washington (DC): National Academies Press (US); 2019 May 16. 2, Adolescent Development.
- PDF version of this title (5.9M)
In this Page
Recent activity.
- Adolescent Development - The Promise of Adolescence Adolescent Development - The Promise of Adolescence
Your browsing activity is empty.
Activity recording is turned off.
Turn recording back on
Connect with NLM
National Library of Medicine 8600 Rockville Pike Bethesda, MD 20894
Web Policies FOIA HHS Vulnerability Disclosure
Help Accessibility Careers

The Power of Personal Problems in Adolescent Life
Problems may be unwanted, but coping with them can strengthen adolescent growth..
Posted January 18, 2022 | Reviewed by Michelle Quirk
- What Is Resilience?
- Take our Resilience Test
- Find a therapist near me
- Three common kinds of adolescent problems are something to solve, something to persevere, and something to suffer.
- A "problem" is a judgment call declaring a discrepancy between how things are and how one would like them to be that causes dissatisfaction.
- Coping with problems can be strengthening when figuring out takes intelligence, when effort takes persistence, or when recovery takes resilience.

Problems can be costly and complicating. They take energy to contend with and make life more demanding: “What must I deal with now?” So, consider problems in three common forms: problems as something to solve, problems as something to persevere, and problems as something to suffer.
Kinds of Problems
- Problems to solve can be confusing : “I don’t know what’s going on or what to do in this situation!” The younger teenager wonders why she wasn’t socially included. Or the older teenager finds functional independence comes with a lot to figure out. These kinds of problems demand to be understood. They prompt the puzzled person to search for a solution or explanation. They arouse curiosity.
- Problems to persevere can take commitment : “I must keep hanging in there!” The young teenager pledges to the slow rehabilitation of a sports injury. Or the older teenager must develop more self-discipline to support growing independence. These kinds of problems can take constant trying. They prompt the beset person to work a difficult or tiresome circumstance through. They create challenge.
- Problems to endure can be painful : “Because of what happened I’m really miserable!” The younger teenager has to deal with loss from his romantic break-up in high school. Or the even older teenager now finds themselves missing the secure comforts of home. These kinds of problems can be unhappy to deal with. They prompt the injured person to feel suffering and sorrow. They require recovery.
And, of course, major problems are often experienced as some mix of these basic three: “Moving and changing schools in seventh grade has upended my life!” Now the young person is figuring out the new middle school, is making every effort to form new relationships, and is sorely missing old friends left behind: “I’ve got problems on top of problems!”
Dealing With Unhappy Problems
To a degree, all unhappy problems are self-made because they are judgment calls about what is or isn’t happening that one decides is not OK. Painful problems are negative comparisons or complaints: “The way things are is not how I want them to be!” This discrepancy can create dissatisfaction that causes unhappiness: “I’m feeling really down about how things turned out!”
In simplest terms, there are only three ways to alleviate unhappiness problems. The person can change how things are to how they want things to be: “I feel better after getting things to go my way.” The person can change how they want things to be to fit how things actually are: “I feel better just adjusting to reality.” The person can do a mix of the two: “I feel better changing what I can and accepting what I can’t.”
Being Problem-Prone
Deciding they have a problem, a young person tells themselves that something needs fixing or changing in their life: “I’m not OK how I am.” At worst: “I'm never going to be like others who I like!” Now they have created a discrepancy between how things are and how they want things to be, thereby breeding dissatisfaction that can motivate corrective action. They may try to change something about themselves or in their world, or they may create an ongoing sense of discontent with themselves if they do not: “What’s the matter with me?” A lot of middle-school adolescents, in the throes of puberty and competition to socially belong, are tormenting themselves with this question, so it's important that parents never ask: "What's wrong with you?"
Confronting a Problem
Young people can sometimes use help choosing their problems wisely: “You may have enough complaints about yourself right now without adding more.” Having said this, it can take courage to declare, confront, and then address a problem. Judging oneself deficient isn’t fun. People tend to be judgmental about how they are and how their life is unfolding: what is going right and wrong, well or badly, succeeding or failing, for example. Declaring a problem can address some deficiency and motivate desire for personal change: “I don’t have any friends!” However, problems don’t just specify something wrong; they can also motivate making something right. “I’m going to be a joiner, not a loner!” So, while problems can inflict pain, they can also motivate progress, sometimes combining a mix of both.
Problems Made by Parents
Parents can add to adolescents' problems. “How can you be OK letting schoolwork go?” asks the baffled parent of the capable young teenager who has given up caring about grades because now "social" feels like it counts more than "academic." One part of parental oversight can be declaring an adolescent problem where the young person wants his life left alone: “Performance now will affect your future opportunities; therefore, we will supervise your homework to see that it gets done.” Conscientious parents are often problem makers this way, sometimes unpopular on this account: “Quit bugging me!” The parents reply, “We are on your side, not against you. Keeping after you is a hard part of our job.”
The Gift of Problems
How should you advise your adolescent about problems? Maybe treat all problems as gifts of adversity—the opportunity to claim hard-earned benefits from coping with obstacles in life.
- Figuring out takes intelligence : “Problem-solving is like cracking a puzzle or fixing what’s wrong.”
- Coping with challenges takes persistence: “Determination requires not giving up until achieving what matters.”
- Recovering from hurt takes resilience : “Getting over injury is like growing from feeling badly to finding how to feel better.”
We may not enjoy the problems in our life, but people often gain capacity from coping with difficulties they bring. Thus, if a young person engaged with significant hardships growing up, she or he may have claimed valuable strengths on that account. Increased intelligence, persistence, and resilience can stand them in good stead as normal frustrations and setbacks of young adulthood unfold.

What the young person discovers is this: When treated as tests, problems are often opportunities in disguise, having much of lasting value to teach from hard-earned experience. A kind of seasoned confidence can result: “Tough times I’ve known have prepared me for tough times ahead. I’ve been there before.”

Carl Pickhardt Ph.D. is a psychologist in private counseling and public lecturing practice in Austin, Texas. His latest book is Holding On While Letting Go: Parenting Your Child Through the Four Freedoms of Adolescence.
- Find a Therapist
- Find a Treatment Center
- Find a Psychiatrist
- Find a Support Group
- Find Online Therapy
- United States
- Brooklyn, NY
- Chicago, IL
- Houston, TX
- Los Angeles, CA
- New York, NY
- Portland, OR
- San Diego, CA
- San Francisco, CA
- Seattle, WA
- Washington, DC
- Asperger's
- Bipolar Disorder
- Chronic Pain
- Eating Disorders
- Passive Aggression
- Personality
- Goal Setting
- Positive Psychology
- Stopping Smoking
- Low Sexual Desire
- Relationships
- Child Development
- Self Tests NEW
- Therapy Center
- Diagnosis Dictionary
- Types of Therapy

Sticking up for yourself is no easy task. But there are concrete skills you can use to hone your assertiveness and advocate for yourself.
- Emotional Intelligence
- Gaslighting
- Affective Forecasting
- Neuroscience
IMAGES
COMMENTS
On Aug 12, we marked International Youth Day. A day to celebrate the potential and contributions of young people, but also to reflect on the barriers and challenges that threaten the health and wellbeing of the 1·3 billion adolescents (16% of the global population) aged 10 to 19 years. Health in adolescence will influence health, wellbeing, and prospects as adults. Adolescence is a critical ...
A 2020 study estimated that as many as 2.9 million children and adolescents in North America have nonverbal learning disability, or NVLD, which affects a person's spatial-visual skills.
Challenges of Parenting Teens Today. 1. Technology and mental health ... JAMA Network, (2022) Trends in Drug Overdose Deaths Among US Adolescents, January 2010 to June 2021.
Elvira K. Gonzalez says there was a lot of beauty to growing up in the culturally rich border town of Laredo, Texas. But there were some challenges, too. Her new memoir, Hurdles in the Dark ...
Indeed, I felt the same way. My relationship with toplessness was part of a very democratic cultural status quo. If every woman on the beaches of the Mediterranean—from the sexy girls tanning on ...
The results are confirmed by robustness analysis and show that greater U.S. fiscal challenges affect negatively the policy rates in both EMEs and DEs, with a greater impact observed in EMEs. Moreover, a low degree of financial repression is associated with more significant spillover effects from greater U.S. fiscal challenges.
Abstract. In recent years, the aviation industry has witnessed a transformative wave of innovation in electrified aircraft propulsion (EAP), driven by sustainability and efficiency goals. Integration of novel electrical subsystems, including high-voltage power electronics, motors/generators, and energy storage devices, has introduced intricate complexities. In this context, an intensified ...
Abstract. The influence of increasing resource scarcity and climate change has a significant impact on aviation. Therefore, the European Commission has set ambitious goals with a 75 % reduction in CO2 and a 90 % reduction in NOX as part of the Flightpath 2050 vision. Achieving these goals requires the use of disruptive technologies in aviation, especially in propulsion. In addition to the use ...
The doctor's death has sparked a nation-wide conversation on violence against women in India The rape and murder of a trainee doctor in India's Kolkata city earlier this month has sparked ...
Public debt ratios in Europe increased significantly in response to the pandemic and energy shocks and have remained higher than before the pandemic in most countries. Going forward, the projected public debt trajectories are broadly flat overall in advanced Europe but have a rising profile in emerging Europe. Government financing needs are still elevated, and the unwinding of quantitative ...
A new challenge for Harris The return of Trump's legal quagmire to center stage presents new challenges for Harris. She has focused the early weeks of her White House bid on the pain Americans ...
Physically, pubescence commences with the onset of puberty, an organic process regulated by hormonal changes that lead to growth spurts, the development of secondary sexual characteristics, the onset of menstruation in girls and the capacity for sperm production in boys.
Problems of Adolescence. By Norman J. Kelman. [In this lecture, Dr. Norman J. Kelman talks about factors affecting the development of a self in adolescence. Topics include: « Discussion of the "development of self" among adolescents. Influence on physical and emotional changes, and the complications of the irregularity of these changes between ...
Adolescence is a time of change: changes to hormones and the body, changes in the social environment, and changes to the brain and the mind. Although most young people develop into healthy adults, adolescence confers vulnerability to mental health problems. Many mental illnesses, including depression, anxiety, eating disorders, substance use disorders, and psychosis, first appear before the ...
CHALLENGES OF ADOLESCENCE. Adolescence is a time in a young person's life where they move from dependency on their parents to independence, autonomy and maturity. The young person begins to move from the family group being their major social system, to the family taking a lesser role and being part of a peer group becomes a greater attraction ...
In the new survey, seven-in-ten teens say anxiety and depression are major problems among their peers - a concern that's shared by mental health researchers and clinicians. Data on the prevalence of anxiety disorders is hard to come by among teens specifically. But 7% of youths ages 3 to 17 had such a condition in 2016-17, according to the ...
By definition, adolescence is "the developmental period of transition from childhood to adulthood; it involves biological cognitive, and socioemotional changes." (Santrock) The word 'adolescence' is from Latin 'adolescere', meaning 'to grow up' and that really what the entire period is all about.
Essay # 1. Meaning of Adolescence: Adolescence is a time of rapid physiological and psychological change of intensive readjustment to the family, school, work and social life and of preparation for adult roles. It starts with puberty and ends with the achievement of an adult work role. It usually begins between 11 and 16 years in boys and ...
Adolescence Essay: Adolescence is the phase of transition between childhood and adulthood. It involves the physical and psychological growth and development of a person during the puberty period and is usually marked by the teenage years. The ages between 10 to 24 are generally said to be adolescence period. During this period, the changes are associated […]
Introduction. First coined by Hall (1904) only a century ago, adolescence was "created" by the convergence of multiple trends, including labor and schooling laws, that extended dependency beyond childhood and delayed entry into adult roles (Modell & Goodman 1990).Adolescence as a period of dependency and preparation for adulthood has since been reinforced through more recent social changes ...
Other physical changes experienced during adolescence include: a. The development of acne which is a serious issue. b. Muscle gain which can sometimes result in increased body weight in adolescents. c. Both boys' and girls' development of pubic hair. d. Body odour becomes apparent.
Stage 5: Adolescence (Ages 12 to 19)—Identity vs. Role Confusion. Adolescence is the stage that bridges childhood and adulthood. Teenagers embark on the transition to becoming adults, attempting ...
Adolescence is a life period that involves many challenges and changes in different areas such as increasing academic demands, rearrangement of relationships with parents and peers, and developing one's own personal identity [10,11]. According to PISA 2015 results on students' well-being, 66% of students across OECD countries report that ...
Adolescence is a transition phase from childhood to adulthood, which is marked by several biological, cognitive, and psychosocial changes. The characteristics which emerge during adolescence involve: a tendency to experiment and seek novel experiences, a heightened sense of vulnerability, a low risk perception, an intense desire for independence, and an inner search for self-identity which ...
Adolescence is the toughest half of growing up-separating from childhood, detaching for independence, and differentiating for individuality. Adolescence requires that parents adjust expectations ...
Adolescence is the period of transition between childhood and adulthood. Children entering adolescence are going through many changes in their bodies and brains. These include physical, intellectual, psychological and social challenges, as well as development of their own moral compass. The changes are rapid and often take place at different rates.
They can affect a teen's usual way of thinking, feeling or acting, and interfere with daily life. Adding to the urgency: Mental health challenges among teens are not uncommon. Up to 75% of mental health challenges emerge during adolescence, and according to the Mental Health First Aid (MHFA) curriculum, one in five teens has had a serious ...
mental health are overlooked for several reasons, such as a. lack of knowledge or awareness of mental health among health. workers and also the stigma that prevent from seeking help. [4] According ...
Adolescence is a period of significant development that begins with the onset of puberty1 and ends in the mid-20s. Consider how different a person is at the age of 12 from the person he or she is at age 24. The trajectory between those two ages involves a profound amount of change in all domains of development—biological, cognitive, psychosocial, and emotional. Personal relationships and ...
Increased intelligence, persistence, and resilience can stand them in good stead as normal frustrations and setbacks of young adulthood unfold. What the young person discovers is this: When ...