- Research Group
- Job Seekers

Research Tips

Understanding the Difference between Research Questions and Objectives
January 13, 2023
When conducting research, clearly understanding the difference between research questions and objectives is important. While these terms are often used interchangeably, they refer to two distinct aspects of the research process.
Research questions are broad statements that guide the overall direction of the research. They identify the main problem or area of inquiry that the research will address. For example, a research question might be, "What is the impact of social media on teenage mental health?" This question sets the stage for the research and helps to define the scope of the study.

- Research questions are more general and open-ended, while objectives are specific and measurable.
- Research questions identify the main problem or area of inquiry, while objectives define the specific outcomes that the researcher is looking to achieve.
- Research questions help define the study's scope, while objectives help guide the research process.
- Research questions are often used to generate hypotheses or identify gaps in existing knowledge, while objectives are used to establish clear and achievable targets for the research.
- Research questions and objectives are not mutually exclusive, but well-defined research questions should lead to specific objectives necessary to answer the question.
On the other hand, research objectives are specific, measurable goals that the research aims to achieve. They are used to guide the research process and help to define the specific outcomes that the researcher is looking to achieve. For example, an objective for the above research question might be "To determine the correlation between social media usage and rates of depression in teenagers." This objective is more specific and measurable than the research question and helps define the specific outcomes that the researcher is looking to achieve.
It is important to note that research questions and objectives are not mutually exclusive; a study can have one or several questions and objectives. A well-defined research question should lead to specific objectives necessary to answer the question.
In summary, research questions and objectives are two distinct aspects of the research process. Research questions are broad statements that guide the overall direction of the research, while research objectives are specific, measurable goals that the research aims to achieve. Understanding these two terms' differences is essential for conducting effective and meaningful research.
Educational resources and simple solutions for your research journey

What Are Research Objectives and How to Write Them (with Examples)
Table of Contents
Introduction
Research is at the center of everything researchers do, and setting clear, well-defined research objectives plays a pivotal role in guiding scholars toward their desired outcomes. Research papers are essential instruments for researchers to effectively communicate their work. Among the many sections that constitute a research paper, the introduction plays a key role in providing a background and setting the context. 1 Research objectives, which define the aims of the study, are usually stated in the introduction. Every study has a research question that the authors are trying to answer, and the objective is an active statement about how the study will answer this research question. These objectives help guide the development and design of the study and steer the research in the appropriate direction; if this is not clearly defined, a project can fail!
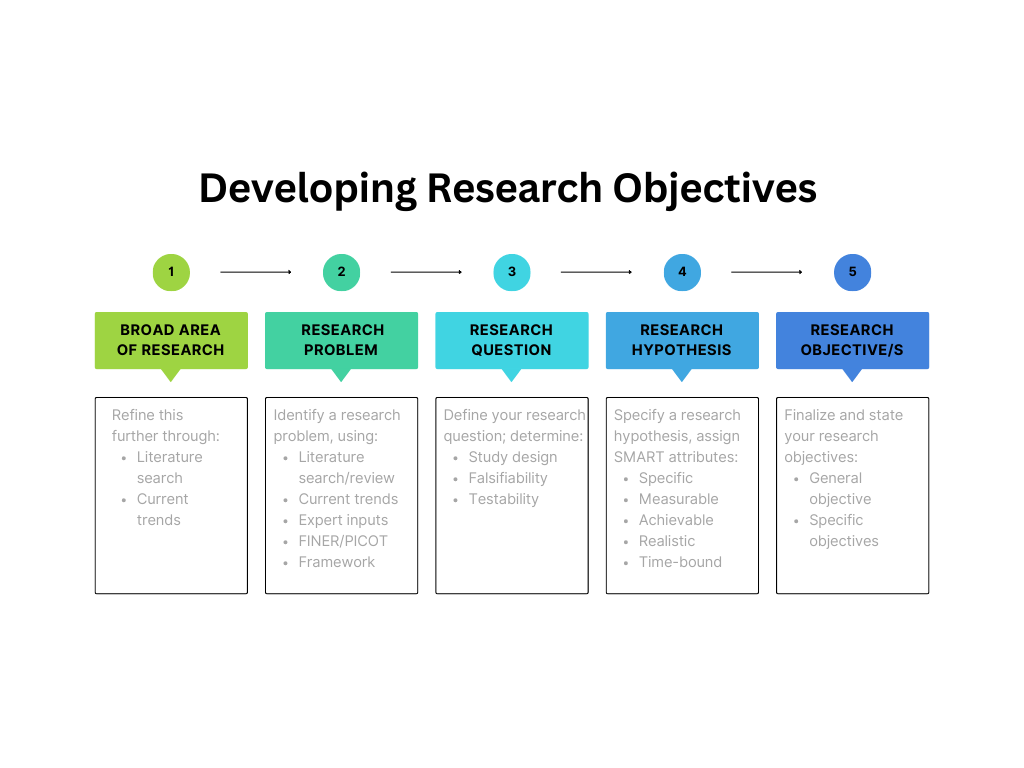
Research studies have a research question, research hypothesis, and one or more research objectives. A research question is what a study aims to answer, and a research hypothesis is a predictive statement about the relationship between two or more variables, which the study sets out to prove or disprove. Objectives are specific, measurable goals that the study aims to achieve. The difference between these three is illustrated by the following example:
- Research question : How does low-intensity pulsed ultrasound (LIPUS) compare with a placebo device in managing the symptoms of skeletally mature patients with patellar tendinopathy?
- Research hypothesis : Pain levels are reduced in patients who receive daily active-LIPUS (treatment) for 12 weeks compared with individuals who receive inactive-LIPUS (placebo).
- Research objective : To investigate the clinical efficacy of LIPUS in the management of patellar tendinopathy symptoms.
This article discusses the importance of clear, well-thought out objectives and suggests methods to write them clearly.
What is the introduction in research papers?
Research objectives are usually included in the introduction section. This section is the first that the readers will read so it is essential that it conveys the subject matter appropriately and is well written to create a good first impression. A good introduction sets the tone of the paper and clearly outlines the contents so that the readers get a quick snapshot of what to expect.
A good introduction should aim to: 2,3
- Indicate the main subject area, its importance, and cite previous literature on the subject
- Define the gap(s) in existing research, ask a research question, and state the objectives
- Announce the present research and outline its novelty and significance
- Avoid repeating the Abstract, providing unnecessary information, and claiming novelty without accurate supporting information.
Why are research objectives important?
Objectives can help you stay focused and steer your research in the required direction. They help define and limit the scope of your research, which is important to efficiently manage your resources and time. The objectives help to create and maintain the overall structure, and specify two main things—the variables and the methods of quantifying the variables.
A good research objective:
- defines the scope of the study
- gives direction to the research
- helps maintain focus and avoid diversions from the topic
- minimizes wastage of resources like time, money, and energy
Types of research objectives
Research objectives can be broadly classified into general and specific objectives . 4 General objectives state what the research expects to achieve overall while specific objectives break this down into smaller, logically connected parts, each of which addresses various parts of the research problem. General objectives are the main goals of the study and are usually fewer in number while specific objectives are more in number because they address several aspects of the research problem.
Example (general objective): To investigate the factors influencing the financial performance of firms listed in the New York Stock Exchange market.
Example (specific objective): To assess the influence of firm size on the financial performance of firms listed in the New York Stock Exchange market.
In addition to this broad classification, research objectives can be grouped into several categories depending on the research problem, as given in Table 1.
Table 1: Types of research objectives
| Exploratory | Explores a previously unstudied topic, issue, or phenomenon; aims to generate ideas or hypotheses |
| Descriptive | Describes the characteristics and features of a particular population or group |
| Explanatory | Explains the relationships between variables; seeks to identify cause-and-effect relationships |
| Predictive | Predicts future outcomes or events based on existing data samples or trends |
| Diagnostic | Identifies factors contributing to a particular problem |
| Comparative | Compares two or more groups or phenomena to identify similarities and differences |
| Historical | Examines past events and trends to understand their significance and impact |
| Methodological | Develops and improves research methods and techniques |
| Theoretical | Tests and refines existing theories or helps develop new theoretical perspectives |
Characteristics of research objectives
Research objectives must start with the word “To” because this helps readers identify the objective in the absence of headings and appropriate sectioning in research papers. 5,6
- A good objective is SMART (mostly applicable to specific objectives):
- Specific—clear about the what, why, when, and how
- Measurable—identifies the main variables of the study and quantifies the targets
- Achievable—attainable using the available time and resources
- Realistic—accurately addresses the scope of the problem
- Time-bound—identifies the time in which each step will be completed
- Research objectives clarify the purpose of research.
- They help understand the relationship and dissimilarities between variables.
- They provide a direction that helps the research to reach a definite conclusion.
How to write research objectives?
Research objectives can be written using the following steps: 7
- State your main research question clearly and concisely.
- Describe the ultimate goal of your study, which is similar to the research question but states the intended outcomes more definitively.
- Divide this main goal into subcategories to develop your objectives.
- Limit the number of objectives (1-2 general; 3-4 specific)
- Assess each objective using the SMART
- Start each objective with an action verb like assess, compare, determine, evaluate, etc., which makes the research appear more actionable.
- Use specific language without making the sentence data heavy.
- The most common section to add the objectives is the introduction and after the problem statement.
- Add the objectives to the abstract (if there is one).
- State the general objective first, followed by the specific objectives.
Formulating research objectives
Formulating research objectives has the following five steps, which could help researchers develop a clear objective: 8
- Identify the research problem.
- Review past studies on subjects similar to your problem statement, that is, studies that use similar methods, variables, etc.
- Identify the research gaps the current study should cover based on your literature review. These gaps could be theoretical, methodological, or conceptual.
- Define the research question(s) based on the gaps identified.
- Revise/relate the research problem based on the defined research question and the gaps identified. This is to confirm that there is an actual need for a study on the subject based on the gaps in literature.
- Identify and write the general and specific objectives.
- Incorporate the objectives into the study.
Advantages of research objectives
Adding clear research objectives has the following advantages: 4,8
- Maintains the focus and direction of the research
- Optimizes allocation of resources with minimal wastage
- Acts as a foundation for defining appropriate research questions and hypotheses
- Provides measurable outcomes that can help evaluate the success of the research
- Determines the feasibility of the research by helping to assess the availability of required resources
- Ensures relevance of the study to the subject and its contribution to existing literature
Disadvantages of research objectives
Research objectives also have few disadvantages, as listed below: 8
- Absence of clearly defined objectives can lead to ambiguity in the research process
- Unintentional bias could affect the validity and accuracy of the research findings
Key takeaways
- Research objectives are concise statements that describe what the research is aiming to achieve.
- They define the scope and direction of the research and maintain focus.
- The objectives should be SMART—specific, measurable, achievable, realistic, and time-bound.
- Clear research objectives help avoid collection of data or resources not required for the study.
- Well-formulated specific objectives help develop the overall research methodology, including data collection, analysis, interpretation, and utilization.
- Research objectives should cover all aspects of the problem statement in a coherent way.
- They should be clearly stated using action verbs.
Frequently asked questions on research objectives
Q: what’s the difference between research objectives and aims 9.
A: Research aims are statements that reflect the broad goal(s) of the study and outline the general direction of the research. They are not specific but clearly define the focus of the study.
Example: This research aims to explore employee experiences of digital transformation in retail HR.
Research objectives focus on the action to be taken to achieve the aims. They make the aims more practical and should be specific and actionable.
Example: To observe the retail HR employees throughout the digital transformation.
Q: What are the examples of research objectives, both general and specific?
A: Here are a few examples of research objectives:
- To identify the antiviral chemical constituents in Mumbukura gitoniensis (general)
- To carry out solvent extraction of dried flowers of Mumbukura gitoniensis and isolate the constituents. (specific)
- To determine the antiviral activity of each of the isolated compounds. (specific)
- To examine the extent, range, and method of coral reef rehabilitation projects in five shallow reef areas adjacent to popular tourist destinations in the Philippines.
- To investigate species richness of mammal communities in five protected areas over the past 20 years.
- To evaluate the potential application of AI techniques for estimating best-corrected visual acuity from fundus photographs with and without ancillary information.
- To investigate whether sport influences psychological parameters in the personality of asthmatic children.
Q: How do I develop research objectives?
A: Developing research objectives begins with defining the problem statement clearly, as illustrated by Figure 1. Objectives specify how the research question will be answered and they determine what is to be measured to test the hypothesis.
Q: Are research objectives measurable?
A: The word “measurable” implies that something is quantifiable. In terms of research objectives, this means that the source and method of collecting data are identified and that all these aspects are feasible for the research. Some metrics can be created to measure your progress toward achieving your objectives.
Q: Can research objectives change during the study?
A: Revising research objectives during the study is acceptable in situations when the selected methodology is not progressing toward achieving the objective, or if there are challenges pertaining to resources, etc. One thing to keep in mind is the time and resources you would have to complete your research after revising the objectives. Thus, as long as your problem statement and hypotheses are unchanged, minor revisions to the research objectives are acceptable.
Q: What is the difference between research questions and research objectives? 10
| Broad statement; guide the overall direction of the research | Specific, measurable goals that the research aims to achieve |
| Identify the main problem | Define the specific outcomes the study aims to achieve |
| Used to generate hypotheses or identify gaps in existing knowledge | Used to establish clear and achievable targets for the research |
| Not mutually exclusive with research objectives | Should be directly related to the research question |
| Example: | Example: |
Q: Are research objectives the same as hypotheses?
A: No, hypotheses are predictive theories that are expressed in general terms. Research objectives, which are more specific, are developed from hypotheses and aim to test them. A hypothesis can be tested using several methods and each method will have different objectives because the methodology to be used could be different. A hypothesis is developed based on observation and reasoning; it is a calculated prediction about why a particular phenomenon is occurring. To test this prediction, different research objectives are formulated. Here’s a simple example of both a research hypothesis and research objective.
Research hypothesis : Employees who arrive at work earlier are more productive.
Research objective : To assess whether employees who arrive at work earlier are more productive.
To summarize, research objectives are an important part of research studies and should be written clearly to effectively communicate your research. We hope this article has given you a brief insight into the importance of using clearly defined research objectives and how to formulate them.
- Farrugia P, Petrisor BA, Farrokhyar F, Bhandari M. Practical tips for surgical research: Research questions, hypotheses and objectives. Can J Surg. 2010 Aug;53(4):278-81.
- Abbadia J. How to write an introduction for a research paper. Mind the Graph website. Accessed June 14, 2023. https://mindthegraph.com/blog/how-to-write-an-introduction-for-a-research-paper/
- Writing a scientific paper: Introduction. UCI libraries website. Accessed June 15, 2023. https://guides.lib.uci.edu/c.php?g=334338&p=2249903
- Research objectives—Types, examples and writing guide. Researchmethod.net website. Accessed June 17, 2023. https://researchmethod.net/research-objectives/#:~:text=They%20provide%20a%20clear%20direction,track%20and%20achieve%20their%20goals .
- Bartle P. SMART Characteristics of good objectives. Community empowerment collective website. Accessed June 16, 2023. https://cec.vcn.bc.ca/cmp/modules/pd-smar.htm
- Research objectives. Studyprobe website. Accessed June 18, 2023. https://www.studyprobe.in/2022/08/research-objectives.html
- Corredor F. How to write objectives in a research paper. wikiHow website. Accessed June 18, 2023. https://www.wikihow.com/Write-Objectives-in-a-Research-Proposal
- Research objectives: Definition, types, characteristics, advantages. AccountingNest website. Accessed June 15, 2023. https://www.accountingnest.com/articles/research/research-objectives
- Phair D., Shaeffer A. Research aims, objectives & questions. GradCoach website. Accessed June 20, 2023. https://gradcoach.com/research-aims-objectives-questions/
- Understanding the difference between research questions and objectives. Accessed June 21, 2023. https://board.researchersjob.com/blog/research-questions-and-objectives
R Discovery is a literature search and research reading platform that accelerates your research discovery journey by keeping you updated on the latest, most relevant scholarly content. With 250M+ research articles sourced from trusted aggregators like CrossRef, Unpaywall, PubMed, PubMed Central, Open Alex and top publishing houses like Springer Nature, JAMA, IOP, Taylor & Francis, NEJM, BMJ, Karger, SAGE, Emerald Publishing and more, R Discovery puts a world of research at your fingertips.
Try R Discovery Prime FREE for 1 week or upgrade at just US$72 a year to access premium features that let you listen to research on the go, read in your language, collaborate with peers, auto sync with reference managers, and much more. Choose a simpler, smarter way to find and read research – Download the app and start your free 7-day trial today !
Related Posts

Research in Shorts: R Discovery’s New Feature Helps Academics Assess Relevant Papers in 2mins

How Does R Discovery’s Interplatform Capability Enhance Research Accessibility

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- J Korean Med Sci
- v.37(16); 2022 Apr 25
A Practical Guide to Writing Quantitative and Qualitative Research Questions and Hypotheses in Scholarly Articles
Edward barroga.
1 Department of General Education, Graduate School of Nursing Science, St. Luke’s International University, Tokyo, Japan.
Glafera Janet Matanguihan
2 Department of Biological Sciences, Messiah University, Mechanicsburg, PA, USA.
The development of research questions and the subsequent hypotheses are prerequisites to defining the main research purpose and specific objectives of a study. Consequently, these objectives determine the study design and research outcome. The development of research questions is a process based on knowledge of current trends, cutting-edge studies, and technological advances in the research field. Excellent research questions are focused and require a comprehensive literature search and in-depth understanding of the problem being investigated. Initially, research questions may be written as descriptive questions which could be developed into inferential questions. These questions must be specific and concise to provide a clear foundation for developing hypotheses. Hypotheses are more formal predictions about the research outcomes. These specify the possible results that may or may not be expected regarding the relationship between groups. Thus, research questions and hypotheses clarify the main purpose and specific objectives of the study, which in turn dictate the design of the study, its direction, and outcome. Studies developed from good research questions and hypotheses will have trustworthy outcomes with wide-ranging social and health implications.
INTRODUCTION
Scientific research is usually initiated by posing evidenced-based research questions which are then explicitly restated as hypotheses. 1 , 2 The hypotheses provide directions to guide the study, solutions, explanations, and expected results. 3 , 4 Both research questions and hypotheses are essentially formulated based on conventional theories and real-world processes, which allow the inception of novel studies and the ethical testing of ideas. 5 , 6
It is crucial to have knowledge of both quantitative and qualitative research 2 as both types of research involve writing research questions and hypotheses. 7 However, these crucial elements of research are sometimes overlooked; if not overlooked, then framed without the forethought and meticulous attention it needs. Planning and careful consideration are needed when developing quantitative or qualitative research, particularly when conceptualizing research questions and hypotheses. 4
There is a continuing need to support researchers in the creation of innovative research questions and hypotheses, as well as for journal articles that carefully review these elements. 1 When research questions and hypotheses are not carefully thought of, unethical studies and poor outcomes usually ensue. Carefully formulated research questions and hypotheses define well-founded objectives, which in turn determine the appropriate design, course, and outcome of the study. This article then aims to discuss in detail the various aspects of crafting research questions and hypotheses, with the goal of guiding researchers as they develop their own. Examples from the authors and peer-reviewed scientific articles in the healthcare field are provided to illustrate key points.
DEFINITIONS AND RELATIONSHIP OF RESEARCH QUESTIONS AND HYPOTHESES
A research question is what a study aims to answer after data analysis and interpretation. The answer is written in length in the discussion section of the paper. Thus, the research question gives a preview of the different parts and variables of the study meant to address the problem posed in the research question. 1 An excellent research question clarifies the research writing while facilitating understanding of the research topic, objective, scope, and limitations of the study. 5
On the other hand, a research hypothesis is an educated statement of an expected outcome. This statement is based on background research and current knowledge. 8 , 9 The research hypothesis makes a specific prediction about a new phenomenon 10 or a formal statement on the expected relationship between an independent variable and a dependent variable. 3 , 11 It provides a tentative answer to the research question to be tested or explored. 4
Hypotheses employ reasoning to predict a theory-based outcome. 10 These can also be developed from theories by focusing on components of theories that have not yet been observed. 10 The validity of hypotheses is often based on the testability of the prediction made in a reproducible experiment. 8
Conversely, hypotheses can also be rephrased as research questions. Several hypotheses based on existing theories and knowledge may be needed to answer a research question. Developing ethical research questions and hypotheses creates a research design that has logical relationships among variables. These relationships serve as a solid foundation for the conduct of the study. 4 , 11 Haphazardly constructed research questions can result in poorly formulated hypotheses and improper study designs, leading to unreliable results. Thus, the formulations of relevant research questions and verifiable hypotheses are crucial when beginning research. 12
CHARACTERISTICS OF GOOD RESEARCH QUESTIONS AND HYPOTHESES
Excellent research questions are specific and focused. These integrate collective data and observations to confirm or refute the subsequent hypotheses. Well-constructed hypotheses are based on previous reports and verify the research context. These are realistic, in-depth, sufficiently complex, and reproducible. More importantly, these hypotheses can be addressed and tested. 13
There are several characteristics of well-developed hypotheses. Good hypotheses are 1) empirically testable 7 , 10 , 11 , 13 ; 2) backed by preliminary evidence 9 ; 3) testable by ethical research 7 , 9 ; 4) based on original ideas 9 ; 5) have evidenced-based logical reasoning 10 ; and 6) can be predicted. 11 Good hypotheses can infer ethical and positive implications, indicating the presence of a relationship or effect relevant to the research theme. 7 , 11 These are initially developed from a general theory and branch into specific hypotheses by deductive reasoning. In the absence of a theory to base the hypotheses, inductive reasoning based on specific observations or findings form more general hypotheses. 10
TYPES OF RESEARCH QUESTIONS AND HYPOTHESES
Research questions and hypotheses are developed according to the type of research, which can be broadly classified into quantitative and qualitative research. We provide a summary of the types of research questions and hypotheses under quantitative and qualitative research categories in Table 1 .
| Quantitative research questions | Quantitative research hypotheses |
|---|---|
| Descriptive research questions | Simple hypothesis |
| Comparative research questions | Complex hypothesis |
| Relationship research questions | Directional hypothesis |
| Non-directional hypothesis | |
| Associative hypothesis | |
| Causal hypothesis | |
| Null hypothesis | |
| Alternative hypothesis | |
| Working hypothesis | |
| Statistical hypothesis | |
| Logical hypothesis | |
| Hypothesis-testing | |
| Qualitative research questions | Qualitative research hypotheses |
| Contextual research questions | Hypothesis-generating |
| Descriptive research questions | |
| Evaluation research questions | |
| Explanatory research questions | |
| Exploratory research questions | |
| Generative research questions | |
| Ideological research questions | |
| Ethnographic research questions | |
| Phenomenological research questions | |
| Grounded theory questions | |
| Qualitative case study questions |
Research questions in quantitative research
In quantitative research, research questions inquire about the relationships among variables being investigated and are usually framed at the start of the study. These are precise and typically linked to the subject population, dependent and independent variables, and research design. 1 Research questions may also attempt to describe the behavior of a population in relation to one or more variables, or describe the characteristics of variables to be measured ( descriptive research questions ). 1 , 5 , 14 These questions may also aim to discover differences between groups within the context of an outcome variable ( comparative research questions ), 1 , 5 , 14 or elucidate trends and interactions among variables ( relationship research questions ). 1 , 5 We provide examples of descriptive, comparative, and relationship research questions in quantitative research in Table 2 .
| Quantitative research questions | |
|---|---|
| Descriptive research question | |
| - Measures responses of subjects to variables | |
| - Presents variables to measure, analyze, or assess | |
| What is the proportion of resident doctors in the hospital who have mastered ultrasonography (response of subjects to a variable) as a diagnostic technique in their clinical training? | |
| Comparative research question | |
| - Clarifies difference between one group with outcome variable and another group without outcome variable | |
| Is there a difference in the reduction of lung metastasis in osteosarcoma patients who received the vitamin D adjunctive therapy (group with outcome variable) compared with osteosarcoma patients who did not receive the vitamin D adjunctive therapy (group without outcome variable)? | |
| - Compares the effects of variables | |
| How does the vitamin D analogue 22-Oxacalcitriol (variable 1) mimic the antiproliferative activity of 1,25-Dihydroxyvitamin D (variable 2) in osteosarcoma cells? | |
| Relationship research question | |
| - Defines trends, association, relationships, or interactions between dependent variable and independent variable | |
| Is there a relationship between the number of medical student suicide (dependent variable) and the level of medical student stress (independent variable) in Japan during the first wave of the COVID-19 pandemic? | |
Hypotheses in quantitative research
In quantitative research, hypotheses predict the expected relationships among variables. 15 Relationships among variables that can be predicted include 1) between a single dependent variable and a single independent variable ( simple hypothesis ) or 2) between two or more independent and dependent variables ( complex hypothesis ). 4 , 11 Hypotheses may also specify the expected direction to be followed and imply an intellectual commitment to a particular outcome ( directional hypothesis ) 4 . On the other hand, hypotheses may not predict the exact direction and are used in the absence of a theory, or when findings contradict previous studies ( non-directional hypothesis ). 4 In addition, hypotheses can 1) define interdependency between variables ( associative hypothesis ), 4 2) propose an effect on the dependent variable from manipulation of the independent variable ( causal hypothesis ), 4 3) state a negative relationship between two variables ( null hypothesis ), 4 , 11 , 15 4) replace the working hypothesis if rejected ( alternative hypothesis ), 15 explain the relationship of phenomena to possibly generate a theory ( working hypothesis ), 11 5) involve quantifiable variables that can be tested statistically ( statistical hypothesis ), 11 6) or express a relationship whose interlinks can be verified logically ( logical hypothesis ). 11 We provide examples of simple, complex, directional, non-directional, associative, causal, null, alternative, working, statistical, and logical hypotheses in quantitative research, as well as the definition of quantitative hypothesis-testing research in Table 3 .
| Quantitative research hypotheses | |
|---|---|
| Simple hypothesis | |
| - Predicts relationship between single dependent variable and single independent variable | |
| If the dose of the new medication (single independent variable) is high, blood pressure (single dependent variable) is lowered. | |
| Complex hypothesis | |
| - Foretells relationship between two or more independent and dependent variables | |
| The higher the use of anticancer drugs, radiation therapy, and adjunctive agents (3 independent variables), the higher would be the survival rate (1 dependent variable). | |
| Directional hypothesis | |
| - Identifies study direction based on theory towards particular outcome to clarify relationship between variables | |
| Privately funded research projects will have a larger international scope (study direction) than publicly funded research projects. | |
| Non-directional hypothesis | |
| - Nature of relationship between two variables or exact study direction is not identified | |
| - Does not involve a theory | |
| Women and men are different in terms of helpfulness. (Exact study direction is not identified) | |
| Associative hypothesis | |
| - Describes variable interdependency | |
| - Change in one variable causes change in another variable | |
| A larger number of people vaccinated against COVID-19 in the region (change in independent variable) will reduce the region’s incidence of COVID-19 infection (change in dependent variable). | |
| Causal hypothesis | |
| - An effect on dependent variable is predicted from manipulation of independent variable | |
| A change into a high-fiber diet (independent variable) will reduce the blood sugar level (dependent variable) of the patient. | |
| Null hypothesis | |
| - A negative statement indicating no relationship or difference between 2 variables | |
| There is no significant difference in the severity of pulmonary metastases between the new drug (variable 1) and the current drug (variable 2). | |
| Alternative hypothesis | |
| - Following a null hypothesis, an alternative hypothesis predicts a relationship between 2 study variables | |
| The new drug (variable 1) is better on average in reducing the level of pain from pulmonary metastasis than the current drug (variable 2). | |
| Working hypothesis | |
| - A hypothesis that is initially accepted for further research to produce a feasible theory | |
| Dairy cows fed with concentrates of different formulations will produce different amounts of milk. | |
| Statistical hypothesis | |
| - Assumption about the value of population parameter or relationship among several population characteristics | |
| - Validity tested by a statistical experiment or analysis | |
| The mean recovery rate from COVID-19 infection (value of population parameter) is not significantly different between population 1 and population 2. | |
| There is a positive correlation between the level of stress at the workplace and the number of suicides (population characteristics) among working people in Japan. | |
| Logical hypothesis | |
| - Offers or proposes an explanation with limited or no extensive evidence | |
| If healthcare workers provide more educational programs about contraception methods, the number of adolescent pregnancies will be less. | |
| Hypothesis-testing (Quantitative hypothesis-testing research) | |
| - Quantitative research uses deductive reasoning. | |
| - This involves the formation of a hypothesis, collection of data in the investigation of the problem, analysis and use of the data from the investigation, and drawing of conclusions to validate or nullify the hypotheses. | |
Research questions in qualitative research
Unlike research questions in quantitative research, research questions in qualitative research are usually continuously reviewed and reformulated. The central question and associated subquestions are stated more than the hypotheses. 15 The central question broadly explores a complex set of factors surrounding the central phenomenon, aiming to present the varied perspectives of participants. 15
There are varied goals for which qualitative research questions are developed. These questions can function in several ways, such as to 1) identify and describe existing conditions ( contextual research question s); 2) describe a phenomenon ( descriptive research questions ); 3) assess the effectiveness of existing methods, protocols, theories, or procedures ( evaluation research questions ); 4) examine a phenomenon or analyze the reasons or relationships between subjects or phenomena ( explanatory research questions ); or 5) focus on unknown aspects of a particular topic ( exploratory research questions ). 5 In addition, some qualitative research questions provide new ideas for the development of theories and actions ( generative research questions ) or advance specific ideologies of a position ( ideological research questions ). 1 Other qualitative research questions may build on a body of existing literature and become working guidelines ( ethnographic research questions ). Research questions may also be broadly stated without specific reference to the existing literature or a typology of questions ( phenomenological research questions ), may be directed towards generating a theory of some process ( grounded theory questions ), or may address a description of the case and the emerging themes ( qualitative case study questions ). 15 We provide examples of contextual, descriptive, evaluation, explanatory, exploratory, generative, ideological, ethnographic, phenomenological, grounded theory, and qualitative case study research questions in qualitative research in Table 4 , and the definition of qualitative hypothesis-generating research in Table 5 .
| Qualitative research questions | |
|---|---|
| Contextual research question | |
| - Ask the nature of what already exists | |
| - Individuals or groups function to further clarify and understand the natural context of real-world problems | |
| What are the experiences of nurses working night shifts in healthcare during the COVID-19 pandemic? (natural context of real-world problems) | |
| Descriptive research question | |
| - Aims to describe a phenomenon | |
| What are the different forms of disrespect and abuse (phenomenon) experienced by Tanzanian women when giving birth in healthcare facilities? | |
| Evaluation research question | |
| - Examines the effectiveness of existing practice or accepted frameworks | |
| How effective are decision aids (effectiveness of existing practice) in helping decide whether to give birth at home or in a healthcare facility? | |
| Explanatory research question | |
| - Clarifies a previously studied phenomenon and explains why it occurs | |
| Why is there an increase in teenage pregnancy (phenomenon) in Tanzania? | |
| Exploratory research question | |
| - Explores areas that have not been fully investigated to have a deeper understanding of the research problem | |
| What factors affect the mental health of medical students (areas that have not yet been fully investigated) during the COVID-19 pandemic? | |
| Generative research question | |
| - Develops an in-depth understanding of people’s behavior by asking ‘how would’ or ‘what if’ to identify problems and find solutions | |
| How would the extensive research experience of the behavior of new staff impact the success of the novel drug initiative? | |
| Ideological research question | |
| - Aims to advance specific ideas or ideologies of a position | |
| Are Japanese nurses who volunteer in remote African hospitals able to promote humanized care of patients (specific ideas or ideologies) in the areas of safe patient environment, respect of patient privacy, and provision of accurate information related to health and care? | |
| Ethnographic research question | |
| - Clarifies peoples’ nature, activities, their interactions, and the outcomes of their actions in specific settings | |
| What are the demographic characteristics, rehabilitative treatments, community interactions, and disease outcomes (nature, activities, their interactions, and the outcomes) of people in China who are suffering from pneumoconiosis? | |
| Phenomenological research question | |
| - Knows more about the phenomena that have impacted an individual | |
| What are the lived experiences of parents who have been living with and caring for children with a diagnosis of autism? (phenomena that have impacted an individual) | |
| Grounded theory question | |
| - Focuses on social processes asking about what happens and how people interact, or uncovering social relationships and behaviors of groups | |
| What are the problems that pregnant adolescents face in terms of social and cultural norms (social processes), and how can these be addressed? | |
| Qualitative case study question | |
| - Assesses a phenomenon using different sources of data to answer “why” and “how” questions | |
| - Considers how the phenomenon is influenced by its contextual situation. | |
| How does quitting work and assuming the role of a full-time mother (phenomenon assessed) change the lives of women in Japan? | |
| Qualitative research hypotheses | |
|---|---|
| Hypothesis-generating (Qualitative hypothesis-generating research) | |
| - Qualitative research uses inductive reasoning. | |
| - This involves data collection from study participants or the literature regarding a phenomenon of interest, using the collected data to develop a formal hypothesis, and using the formal hypothesis as a framework for testing the hypothesis. | |
| - Qualitative exploratory studies explore areas deeper, clarifying subjective experience and allowing formulation of a formal hypothesis potentially testable in a future quantitative approach. | |
Qualitative studies usually pose at least one central research question and several subquestions starting with How or What . These research questions use exploratory verbs such as explore or describe . These also focus on one central phenomenon of interest, and may mention the participants and research site. 15
Hypotheses in qualitative research
Hypotheses in qualitative research are stated in the form of a clear statement concerning the problem to be investigated. Unlike in quantitative research where hypotheses are usually developed to be tested, qualitative research can lead to both hypothesis-testing and hypothesis-generating outcomes. 2 When studies require both quantitative and qualitative research questions, this suggests an integrative process between both research methods wherein a single mixed-methods research question can be developed. 1
FRAMEWORKS FOR DEVELOPING RESEARCH QUESTIONS AND HYPOTHESES
Research questions followed by hypotheses should be developed before the start of the study. 1 , 12 , 14 It is crucial to develop feasible research questions on a topic that is interesting to both the researcher and the scientific community. This can be achieved by a meticulous review of previous and current studies to establish a novel topic. Specific areas are subsequently focused on to generate ethical research questions. The relevance of the research questions is evaluated in terms of clarity of the resulting data, specificity of the methodology, objectivity of the outcome, depth of the research, and impact of the study. 1 , 5 These aspects constitute the FINER criteria (i.e., Feasible, Interesting, Novel, Ethical, and Relevant). 1 Clarity and effectiveness are achieved if research questions meet the FINER criteria. In addition to the FINER criteria, Ratan et al. described focus, complexity, novelty, feasibility, and measurability for evaluating the effectiveness of research questions. 14
The PICOT and PEO frameworks are also used when developing research questions. 1 The following elements are addressed in these frameworks, PICOT: P-population/patients/problem, I-intervention or indicator being studied, C-comparison group, O-outcome of interest, and T-timeframe of the study; PEO: P-population being studied, E-exposure to preexisting conditions, and O-outcome of interest. 1 Research questions are also considered good if these meet the “FINERMAPS” framework: Feasible, Interesting, Novel, Ethical, Relevant, Manageable, Appropriate, Potential value/publishable, and Systematic. 14
As we indicated earlier, research questions and hypotheses that are not carefully formulated result in unethical studies or poor outcomes. To illustrate this, we provide some examples of ambiguous research question and hypotheses that result in unclear and weak research objectives in quantitative research ( Table 6 ) 16 and qualitative research ( Table 7 ) 17 , and how to transform these ambiguous research question(s) and hypothesis(es) into clear and good statements.
| Variables | Unclear and weak statement (Statement 1) | Clear and good statement (Statement 2) | Points to avoid |
|---|---|---|---|
| Research question | Which is more effective between smoke moxibustion and smokeless moxibustion? | “Moreover, regarding smoke moxibustion versus smokeless moxibustion, it remains unclear which is more effective, safe, and acceptable to pregnant women, and whether there is any difference in the amount of heat generated.” | 1) Vague and unfocused questions |
| 2) Closed questions simply answerable by yes or no | |||
| 3) Questions requiring a simple choice | |||
| Hypothesis | The smoke moxibustion group will have higher cephalic presentation. | “Hypothesis 1. The smoke moxibustion stick group (SM group) and smokeless moxibustion stick group (-SLM group) will have higher rates of cephalic presentation after treatment than the control group. | 1) Unverifiable hypotheses |
| Hypothesis 2. The SM group and SLM group will have higher rates of cephalic presentation at birth than the control group. | 2) Incompletely stated groups of comparison | ||
| Hypothesis 3. There will be no significant differences in the well-being of the mother and child among the three groups in terms of the following outcomes: premature birth, premature rupture of membranes (PROM) at < 37 weeks, Apgar score < 7 at 5 min, umbilical cord blood pH < 7.1, admission to neonatal intensive care unit (NICU), and intrauterine fetal death.” | 3) Insufficiently described variables or outcomes | ||
| Research objective | To determine which is more effective between smoke moxibustion and smokeless moxibustion. | “The specific aims of this pilot study were (a) to compare the effects of smoke moxibustion and smokeless moxibustion treatments with the control group as a possible supplement to ECV for converting breech presentation to cephalic presentation and increasing adherence to the newly obtained cephalic position, and (b) to assess the effects of these treatments on the well-being of the mother and child.” | 1) Poor understanding of the research question and hypotheses |
| 2) Insufficient description of population, variables, or study outcomes |
a These statements were composed for comparison and illustrative purposes only.
b These statements are direct quotes from Higashihara and Horiuchi. 16
| Variables | Unclear and weak statement (Statement 1) | Clear and good statement (Statement 2) | Points to avoid |
|---|---|---|---|
| Research question | Does disrespect and abuse (D&A) occur in childbirth in Tanzania? | How does disrespect and abuse (D&A) occur and what are the types of physical and psychological abuses observed in midwives’ actual care during facility-based childbirth in urban Tanzania? | 1) Ambiguous or oversimplistic questions |
| 2) Questions unverifiable by data collection and analysis | |||
| Hypothesis | Disrespect and abuse (D&A) occur in childbirth in Tanzania. | Hypothesis 1: Several types of physical and psychological abuse by midwives in actual care occur during facility-based childbirth in urban Tanzania. | 1) Statements simply expressing facts |
| Hypothesis 2: Weak nursing and midwifery management contribute to the D&A of women during facility-based childbirth in urban Tanzania. | 2) Insufficiently described concepts or variables | ||
| Research objective | To describe disrespect and abuse (D&A) in childbirth in Tanzania. | “This study aimed to describe from actual observations the respectful and disrespectful care received by women from midwives during their labor period in two hospitals in urban Tanzania.” | 1) Statements unrelated to the research question and hypotheses |
| 2) Unattainable or unexplorable objectives |
a This statement is a direct quote from Shimoda et al. 17
The other statements were composed for comparison and illustrative purposes only.
CONSTRUCTING RESEARCH QUESTIONS AND HYPOTHESES
To construct effective research questions and hypotheses, it is very important to 1) clarify the background and 2) identify the research problem at the outset of the research, within a specific timeframe. 9 Then, 3) review or conduct preliminary research to collect all available knowledge about the possible research questions by studying theories and previous studies. 18 Afterwards, 4) construct research questions to investigate the research problem. Identify variables to be accessed from the research questions 4 and make operational definitions of constructs from the research problem and questions. Thereafter, 5) construct specific deductive or inductive predictions in the form of hypotheses. 4 Finally, 6) state the study aims . This general flow for constructing effective research questions and hypotheses prior to conducting research is shown in Fig. 1 .

Research questions are used more frequently in qualitative research than objectives or hypotheses. 3 These questions seek to discover, understand, explore or describe experiences by asking “What” or “How.” The questions are open-ended to elicit a description rather than to relate variables or compare groups. The questions are continually reviewed, reformulated, and changed during the qualitative study. 3 Research questions are also used more frequently in survey projects than hypotheses in experiments in quantitative research to compare variables and their relationships.
Hypotheses are constructed based on the variables identified and as an if-then statement, following the template, ‘If a specific action is taken, then a certain outcome is expected.’ At this stage, some ideas regarding expectations from the research to be conducted must be drawn. 18 Then, the variables to be manipulated (independent) and influenced (dependent) are defined. 4 Thereafter, the hypothesis is stated and refined, and reproducible data tailored to the hypothesis are identified, collected, and analyzed. 4 The hypotheses must be testable and specific, 18 and should describe the variables and their relationships, the specific group being studied, and the predicted research outcome. 18 Hypotheses construction involves a testable proposition to be deduced from theory, and independent and dependent variables to be separated and measured separately. 3 Therefore, good hypotheses must be based on good research questions constructed at the start of a study or trial. 12
In summary, research questions are constructed after establishing the background of the study. Hypotheses are then developed based on the research questions. Thus, it is crucial to have excellent research questions to generate superior hypotheses. In turn, these would determine the research objectives and the design of the study, and ultimately, the outcome of the research. 12 Algorithms for building research questions and hypotheses are shown in Fig. 2 for quantitative research and in Fig. 3 for qualitative research.

EXAMPLES OF RESEARCH QUESTIONS FROM PUBLISHED ARTICLES
- EXAMPLE 1. Descriptive research question (quantitative research)
- - Presents research variables to be assessed (distinct phenotypes and subphenotypes)
- “BACKGROUND: Since COVID-19 was identified, its clinical and biological heterogeneity has been recognized. Identifying COVID-19 phenotypes might help guide basic, clinical, and translational research efforts.
- RESEARCH QUESTION: Does the clinical spectrum of patients with COVID-19 contain distinct phenotypes and subphenotypes? ” 19
- EXAMPLE 2. Relationship research question (quantitative research)
- - Shows interactions between dependent variable (static postural control) and independent variable (peripheral visual field loss)
- “Background: Integration of visual, vestibular, and proprioceptive sensations contributes to postural control. People with peripheral visual field loss have serious postural instability. However, the directional specificity of postural stability and sensory reweighting caused by gradual peripheral visual field loss remain unclear.
- Research question: What are the effects of peripheral visual field loss on static postural control ?” 20
- EXAMPLE 3. Comparative research question (quantitative research)
- - Clarifies the difference among groups with an outcome variable (patients enrolled in COMPERA with moderate PH or severe PH in COPD) and another group without the outcome variable (patients with idiopathic pulmonary arterial hypertension (IPAH))
- “BACKGROUND: Pulmonary hypertension (PH) in COPD is a poorly investigated clinical condition.
- RESEARCH QUESTION: Which factors determine the outcome of PH in COPD?
- STUDY DESIGN AND METHODS: We analyzed the characteristics and outcome of patients enrolled in the Comparative, Prospective Registry of Newly Initiated Therapies for Pulmonary Hypertension (COMPERA) with moderate or severe PH in COPD as defined during the 6th PH World Symposium who received medical therapy for PH and compared them with patients with idiopathic pulmonary arterial hypertension (IPAH) .” 21
- EXAMPLE 4. Exploratory research question (qualitative research)
- - Explores areas that have not been fully investigated (perspectives of families and children who receive care in clinic-based child obesity treatment) to have a deeper understanding of the research problem
- “Problem: Interventions for children with obesity lead to only modest improvements in BMI and long-term outcomes, and data are limited on the perspectives of families of children with obesity in clinic-based treatment. This scoping review seeks to answer the question: What is known about the perspectives of families and children who receive care in clinic-based child obesity treatment? This review aims to explore the scope of perspectives reported by families of children with obesity who have received individualized outpatient clinic-based obesity treatment.” 22
- EXAMPLE 5. Relationship research question (quantitative research)
- - Defines interactions between dependent variable (use of ankle strategies) and independent variable (changes in muscle tone)
- “Background: To maintain an upright standing posture against external disturbances, the human body mainly employs two types of postural control strategies: “ankle strategy” and “hip strategy.” While it has been reported that the magnitude of the disturbance alters the use of postural control strategies, it has not been elucidated how the level of muscle tone, one of the crucial parameters of bodily function, determines the use of each strategy. We have previously confirmed using forward dynamics simulations of human musculoskeletal models that an increased muscle tone promotes the use of ankle strategies. The objective of the present study was to experimentally evaluate a hypothesis: an increased muscle tone promotes the use of ankle strategies. Research question: Do changes in the muscle tone affect the use of ankle strategies ?” 23
EXAMPLES OF HYPOTHESES IN PUBLISHED ARTICLES
- EXAMPLE 1. Working hypothesis (quantitative research)
- - A hypothesis that is initially accepted for further research to produce a feasible theory
- “As fever may have benefit in shortening the duration of viral illness, it is plausible to hypothesize that the antipyretic efficacy of ibuprofen may be hindering the benefits of a fever response when taken during the early stages of COVID-19 illness .” 24
- “In conclusion, it is plausible to hypothesize that the antipyretic efficacy of ibuprofen may be hindering the benefits of a fever response . The difference in perceived safety of these agents in COVID-19 illness could be related to the more potent efficacy to reduce fever with ibuprofen compared to acetaminophen. Compelling data on the benefit of fever warrant further research and review to determine when to treat or withhold ibuprofen for early stage fever for COVID-19 and other related viral illnesses .” 24
- EXAMPLE 2. Exploratory hypothesis (qualitative research)
- - Explores particular areas deeper to clarify subjective experience and develop a formal hypothesis potentially testable in a future quantitative approach
- “We hypothesized that when thinking about a past experience of help-seeking, a self distancing prompt would cause increased help-seeking intentions and more favorable help-seeking outcome expectations .” 25
- “Conclusion
- Although a priori hypotheses were not supported, further research is warranted as results indicate the potential for using self-distancing approaches to increasing help-seeking among some people with depressive symptomatology.” 25
- EXAMPLE 3. Hypothesis-generating research to establish a framework for hypothesis testing (qualitative research)
- “We hypothesize that compassionate care is beneficial for patients (better outcomes), healthcare systems and payers (lower costs), and healthcare providers (lower burnout). ” 26
- Compassionomics is the branch of knowledge and scientific study of the effects of compassionate healthcare. Our main hypotheses are that compassionate healthcare is beneficial for (1) patients, by improving clinical outcomes, (2) healthcare systems and payers, by supporting financial sustainability, and (3) HCPs, by lowering burnout and promoting resilience and well-being. The purpose of this paper is to establish a scientific framework for testing the hypotheses above . If these hypotheses are confirmed through rigorous research, compassionomics will belong in the science of evidence-based medicine, with major implications for all healthcare domains.” 26
- EXAMPLE 4. Statistical hypothesis (quantitative research)
- - An assumption is made about the relationship among several population characteristics ( gender differences in sociodemographic and clinical characteristics of adults with ADHD ). Validity is tested by statistical experiment or analysis ( chi-square test, Students t-test, and logistic regression analysis)
- “Our research investigated gender differences in sociodemographic and clinical characteristics of adults with ADHD in a Japanese clinical sample. Due to unique Japanese cultural ideals and expectations of women's behavior that are in opposition to ADHD symptoms, we hypothesized that women with ADHD experience more difficulties and present more dysfunctions than men . We tested the following hypotheses: first, women with ADHD have more comorbidities than men with ADHD; second, women with ADHD experience more social hardships than men, such as having less full-time employment and being more likely to be divorced.” 27
- “Statistical Analysis
- ( text omitted ) Between-gender comparisons were made using the chi-squared test for categorical variables and Students t-test for continuous variables…( text omitted ). A logistic regression analysis was performed for employment status, marital status, and comorbidity to evaluate the independent effects of gender on these dependent variables.” 27
EXAMPLES OF HYPOTHESIS AS WRITTEN IN PUBLISHED ARTICLES IN RELATION TO OTHER PARTS
- EXAMPLE 1. Background, hypotheses, and aims are provided
- “Pregnant women need skilled care during pregnancy and childbirth, but that skilled care is often delayed in some countries …( text omitted ). The focused antenatal care (FANC) model of WHO recommends that nurses provide information or counseling to all pregnant women …( text omitted ). Job aids are visual support materials that provide the right kind of information using graphics and words in a simple and yet effective manner. When nurses are not highly trained or have many work details to attend to, these job aids can serve as a content reminder for the nurses and can be used for educating their patients (Jennings, Yebadokpo, Affo, & Agbogbe, 2010) ( text omitted ). Importantly, additional evidence is needed to confirm how job aids can further improve the quality of ANC counseling by health workers in maternal care …( text omitted )” 28
- “ This has led us to hypothesize that the quality of ANC counseling would be better if supported by job aids. Consequently, a better quality of ANC counseling is expected to produce higher levels of awareness concerning the danger signs of pregnancy and a more favorable impression of the caring behavior of nurses .” 28
- “This study aimed to examine the differences in the responses of pregnant women to a job aid-supported intervention during ANC visit in terms of 1) their understanding of the danger signs of pregnancy and 2) their impression of the caring behaviors of nurses to pregnant women in rural Tanzania.” 28
- EXAMPLE 2. Background, hypotheses, and aims are provided
- “We conducted a two-arm randomized controlled trial (RCT) to evaluate and compare changes in salivary cortisol and oxytocin levels of first-time pregnant women between experimental and control groups. The women in the experimental group touched and held an infant for 30 min (experimental intervention protocol), whereas those in the control group watched a DVD movie of an infant (control intervention protocol). The primary outcome was salivary cortisol level and the secondary outcome was salivary oxytocin level.” 29
- “ We hypothesize that at 30 min after touching and holding an infant, the salivary cortisol level will significantly decrease and the salivary oxytocin level will increase in the experimental group compared with the control group .” 29
- EXAMPLE 3. Background, aim, and hypothesis are provided
- “In countries where the maternal mortality ratio remains high, antenatal education to increase Birth Preparedness and Complication Readiness (BPCR) is considered one of the top priorities [1]. BPCR includes birth plans during the antenatal period, such as the birthplace, birth attendant, transportation, health facility for complications, expenses, and birth materials, as well as family coordination to achieve such birth plans. In Tanzania, although increasing, only about half of all pregnant women attend an antenatal clinic more than four times [4]. Moreover, the information provided during antenatal care (ANC) is insufficient. In the resource-poor settings, antenatal group education is a potential approach because of the limited time for individual counseling at antenatal clinics.” 30
- “This study aimed to evaluate an antenatal group education program among pregnant women and their families with respect to birth-preparedness and maternal and infant outcomes in rural villages of Tanzania.” 30
- “ The study hypothesis was if Tanzanian pregnant women and their families received a family-oriented antenatal group education, they would (1) have a higher level of BPCR, (2) attend antenatal clinic four or more times, (3) give birth in a health facility, (4) have less complications of women at birth, and (5) have less complications and deaths of infants than those who did not receive the education .” 30
Research questions and hypotheses are crucial components to any type of research, whether quantitative or qualitative. These questions should be developed at the very beginning of the study. Excellent research questions lead to superior hypotheses, which, like a compass, set the direction of research, and can often determine the successful conduct of the study. Many research studies have floundered because the development of research questions and subsequent hypotheses was not given the thought and meticulous attention needed. The development of research questions and hypotheses is an iterative process based on extensive knowledge of the literature and insightful grasp of the knowledge gap. Focused, concise, and specific research questions provide a strong foundation for constructing hypotheses which serve as formal predictions about the research outcomes. Research questions and hypotheses are crucial elements of research that should not be overlooked. They should be carefully thought of and constructed when planning research. This avoids unethical studies and poor outcomes by defining well-founded objectives that determine the design, course, and outcome of the study.
Disclosure: The authors have no potential conflicts of interest to disclose.
Author Contributions:
- Conceptualization: Barroga E, Matanguihan GJ.
- Methodology: Barroga E, Matanguihan GJ.
- Writing - original draft: Barroga E, Matanguihan GJ.
- Writing - review & editing: Barroga E, Matanguihan GJ.
Research Question 101 📖
Everything you need to know to write a high-quality research question
By: Derek Jansen (MBA) | Reviewed By: Dr. Eunice Rautenbach | October 2023
If you’ve landed on this page, you’re probably asking yourself, “ What is a research question? ”. Well, you’ve come to the right place. In this post, we’ll explain what a research question is , how it’s differen t from a research aim, and how to craft a high-quality research question that sets you up for success.
Research Question 101
What is a research question.
- Research questions vs research aims
- The 4 types of research questions
- How to write a research question
- Frequently asked questions
- Examples of research questions
As the name suggests, the research question is the core question (or set of questions) that your study will (attempt to) answer .
In many ways, a research question is akin to a target in archery . Without a clear target, you won’t know where to concentrate your efforts and focus. Essentially, your research question acts as the guiding light throughout your project and informs every choice you make along the way.
Let’s look at some examples:
What impact does social media usage have on the mental health of teenagers in New York?
How does the introduction of a minimum wage affect employment levels in small businesses in outer London?
How does the portrayal of women in 19th-century American literature reflect the societal attitudes of the time?
What are the long-term effects of intermittent fasting on heart health in adults?
As you can see in these examples, research questions are clear, specific questions that can be feasibly answered within a study. These are important attributes and we’ll discuss each of them in more detail a little later . If you’d like to see more examples of research questions, you can find our RQ mega-list here .

Research Questions vs Research Aims
At this point, you might be asking yourself, “ How is a research question different from a research aim? ”. Within any given study, the research aim and research question (or questions) are tightly intertwined , but they are separate things . Let’s unpack that a little.
A research aim is typically broader in nature and outlines what you hope to achieve with your research. It doesn’t ask a specific question but rather gives a summary of what you intend to explore.
The research question, on the other hand, is much more focused . It’s the specific query you’re setting out to answer. It narrows down the research aim into a detailed, researchable question that will guide your study’s methods and analysis.
Let’s look at an example:
Research Aim: To explore the effects of climate change on marine life in Southern Africa.
Research Question: How does ocean acidification caused by climate change affect the reproduction rates of coral reefs?
As you can see, the research aim gives you a general focus , while the research question details exactly what you want to find out.
Need a helping hand?
Types of research questions
Now that we’ve defined what a research question is, let’s look at the different types of research questions that you might come across. Broadly speaking, there are (at least) four different types of research questions – descriptive , comparative , relational , and explanatory .
Descriptive questions ask what is happening. In other words, they seek to describe a phenomena or situation . An example of a descriptive research question could be something like “What types of exercise do high-performing UK executives engage in?”. This would likely be a bit too basic to form an interesting study, but as you can see, the research question is just focused on the what – in other words, it just describes the situation.
Comparative research questions , on the other hand, look to understand the way in which two or more things differ , or how they’re similar. An example of a comparative research question might be something like “How do exercise preferences vary between middle-aged men across three American cities?”. As you can see, this question seeks to compare the differences (or similarities) in behaviour between different groups.
Next up, we’ve got exploratory research questions , which ask why or how is something happening. While the other types of questions we looked at focused on the what, exploratory research questions are interested in the why and how . As an example, an exploratory research question might ask something like “Why have bee populations declined in Germany over the last 5 years?”. As you can, this question is aimed squarely at the why, rather than the what.
Last but not least, we have relational research questions . As the name suggests, these types of research questions seek to explore the relationships between variables . Here, an example could be something like “What is the relationship between X and Y” or “Does A have an impact on B”. As you can see, these types of research questions are interested in understanding how constructs or variables are connected , and perhaps, whether one thing causes another.
Of course, depending on how fine-grained you want to get, you can argue that there are many more types of research questions , but these four categories give you a broad idea of the different flavours that exist out there. It’s also worth pointing out that a research question doesn’t need to fit perfectly into one category – in many cases, a research question might overlap into more than just one category and that’s okay.
The key takeaway here is that research questions can take many different forms , and it’s useful to understand the nature of your research question so that you can align your research methodology accordingly.

How To Write A Research Question
As we alluded earlier, a well-crafted research question needs to possess very specific attributes, including focus , clarity and feasibility . But that’s not all – a rock-solid research question also needs to be rooted and aligned . Let’s look at each of these.
A strong research question typically has a single focus. So, don’t try to cram multiple questions into one research question; rather split them up into separate questions (or even subquestions), each with their own specific focus. As a rule of thumb, narrow beats broad when it comes to research questions.
Clear and specific
A good research question is clear and specific, not vague and broad. State clearly exactly what you want to find out so that any reader can quickly understand what you’re looking to achieve with your study. Along the same vein, try to avoid using bulky language and jargon – aim for clarity.
Unfortunately, even a super tantalising and thought-provoking research question has little value if you cannot feasibly answer it. So, think about the methodological implications of your research question while you’re crafting it. Most importantly, make sure that you know exactly what data you’ll need (primary or secondary) and how you’ll analyse that data.
A good research question (and a research topic, more broadly) should be rooted in a clear research gap and research problem . Without a well-defined research gap, you risk wasting your effort pursuing a question that’s already been adequately answered (and agreed upon) by the research community. A well-argued research gap lays at the heart of a valuable study, so make sure you have your gap clearly articulated and that your research question directly links to it.
As we mentioned earlier, your research aim and research question are (or at least, should be) tightly linked. So, make sure that your research question (or set of questions) aligns with your research aim . If not, you’ll need to revise one of the two to achieve this.
FAQ: Research Questions
Research question faqs, how many research questions should i have, what should i avoid when writing a research question, can a research question be a statement.
Typically, a research question is phrased as a question, not a statement. A question clearly indicates what you’re setting out to discover.
Can a research question be too broad or too narrow?
Yes. A question that’s too broad makes your research unfocused, while a question that’s too narrow limits the scope of your study.
Here’s an example of a research question that’s too broad:
“Why is mental health important?”
Conversely, here’s an example of a research question that’s likely too narrow:
“What is the impact of sleep deprivation on the exam scores of 19-year-old males in London studying maths at The Open University?”
Can I change my research question during the research process?
How do i know if my research question is good.
A good research question is focused, specific, practical, rooted in a research gap, and aligned with the research aim. If your question meets these criteria, it’s likely a strong question.
Is a research question similar to a hypothesis?
Not quite. A hypothesis is a testable statement that predicts an outcome, while a research question is a query that you’re trying to answer through your study. Naturally, there can be linkages between a study’s research questions and hypothesis, but they serve different functions.
How are research questions and research objectives related?
The research question is a focused and specific query that your study aims to answer. It’s the central issue you’re investigating. The research objective, on the other hand, outlines the steps you’ll take to answer your research question. Research objectives are often more action-oriented and can be broken down into smaller tasks that guide your research process. In a sense, they’re something of a roadmap that helps you answer your research question.
Need some inspiration?
If you’d like to see more examples of research questions, check out our research question mega list here . Alternatively, if you’d like 1-on-1 help developing a high-quality research question, consider our private coaching service .

Psst... there’s more!
This post was based on one of our popular Research Bootcamps . If you're working on a research project, you'll definitely want to check this out ...
Submit a Comment Cancel reply
Your email address will not be published. Required fields are marked *
Save my name, email, and website in this browser for the next time I comment.
- Print Friendly
- Aims and Objectives – A Guide for Academic Writing
- Doing a PhD
One of the most important aspects of a thesis, dissertation or research paper is the correct formulation of the aims and objectives. This is because your aims and objectives will establish the scope, depth and direction that your research will ultimately take. An effective set of aims and objectives will give your research focus and your reader clarity, with your aims indicating what is to be achieved, and your objectives indicating how it will be achieved.
Introduction
There is no getting away from the importance of the aims and objectives in determining the success of your research project. Unfortunately, however, it is an aspect that many students struggle with, and ultimately end up doing poorly. Given their importance, if you suspect that there is even the smallest possibility that you belong to this group of students, we strongly recommend you read this page in full.
This page describes what research aims and objectives are, how they differ from each other, how to write them correctly, and the common mistakes students make and how to avoid them. An example of a good aim and objectives from a past thesis has also been deconstructed to help your understanding.
What Are Aims and Objectives?
Research aims.
A research aim describes the main goal or the overarching purpose of your research project.
In doing so, it acts as a focal point for your research and provides your readers with clarity as to what your study is all about. Because of this, research aims are almost always located within its own subsection under the introduction section of a research document, regardless of whether it’s a thesis , a dissertation, or a research paper .
A research aim is usually formulated as a broad statement of the main goal of the research and can range in length from a single sentence to a short paragraph. Although the exact format may vary according to preference, they should all describe why your research is needed (i.e. the context), what it sets out to accomplish (the actual aim) and, briefly, how it intends to accomplish it (overview of your objectives).
To give an example, we have extracted the following research aim from a real PhD thesis:
Example of a Research Aim
The role of diametrical cup deformation as a factor to unsatisfactory implant performance has not been widely reported. The aim of this thesis was to gain an understanding of the diametrical deformation behaviour of acetabular cups and shells following impaction into the reamed acetabulum. The influence of a range of factors on deformation was investigated to ascertain if cup and shell deformation may be high enough to potentially contribute to early failure and high wear rates in metal-on-metal implants.
Note: Extracted with permission from thesis titled “T he Impact And Deformation Of Press-Fit Metal Acetabular Components ” produced by Dr H Hothi of previously Queen Mary University of London.
Research Objectives
Where a research aim specifies what your study will answer, research objectives specify how your study will answer it.
They divide your research aim into several smaller parts, each of which represents a key section of your research project. As a result, almost all research objectives take the form of a numbered list, with each item usually receiving its own chapter in a dissertation or thesis.
Following the example of the research aim shared above, here are it’s real research objectives as an example:
Example of a Research Objective
- Develop finite element models using explicit dynamics to mimic mallet blows during cup/shell insertion, initially using simplified experimentally validated foam models to represent the acetabulum.
- Investigate the number, velocity and position of impacts needed to insert a cup.
- Determine the relationship between the size of interference between the cup and cavity and deformation for different cup types.
- Investigate the influence of non-uniform cup support and varying the orientation of the component in the cavity on deformation.
- Examine the influence of errors during reaming of the acetabulum which introduce ovality to the cavity.
- Determine the relationship between changes in the geometry of the component and deformation for different cup designs.
- Develop three dimensional pelvis models with non-uniform bone material properties from a range of patients with varying bone quality.
- Use the key parameters that influence deformation, as identified in the foam models to determine the range of deformations that may occur clinically using the anatomic models and if these deformations are clinically significant.
It’s worth noting that researchers sometimes use research questions instead of research objectives, or in other cases both. From a high-level perspective, research questions and research objectives make the same statements, but just in different formats.
Taking the first three research objectives as an example, they can be restructured into research questions as follows:
Restructuring Research Objectives as Research Questions
- Can finite element models using simplified experimentally validated foam models to represent the acetabulum together with explicit dynamics be used to mimic mallet blows during cup/shell insertion?
- What is the number, velocity and position of impacts needed to insert a cup?
- What is the relationship between the size of interference between the cup and cavity and deformation for different cup types?
Difference Between Aims and Objectives
Hopefully the above explanations make clear the differences between aims and objectives, but to clarify:
- The research aim focus on what the research project is intended to achieve; research objectives focus on how the aim will be achieved.
- Research aims are relatively broad; research objectives are specific.
- Research aims focus on a project’s long-term outcomes; research objectives focus on its immediate, short-term outcomes.
- A research aim can be written in a single sentence or short paragraph; research objectives should be written as a numbered list.
How to Write Aims and Objectives
Before we discuss how to write a clear set of research aims and objectives, we should make it clear that there is no single way they must be written. Each researcher will approach their aims and objectives slightly differently, and often your supervisor will influence the formulation of yours on the basis of their own preferences.
Regardless, there are some basic principles that you should observe for good practice; these principles are described below.
Your aim should be made up of three parts that answer the below questions:
- Why is this research required?
- What is this research about?
- How are you going to do it?
The easiest way to achieve this would be to address each question in its own sentence, although it does not matter whether you combine them or write multiple sentences for each, the key is to address each one.
The first question, why , provides context to your research project, the second question, what , describes the aim of your research, and the last question, how , acts as an introduction to your objectives which will immediately follow.
Scroll through the image set below to see the ‘why, what and how’ associated with our research aim example.

Note: Your research aims need not be limited to one. Some individuals per to define one broad ‘overarching aim’ of a project and then adopt two or three specific research aims for their thesis or dissertation. Remember, however, that in order for your assessors to consider your research project complete, you will need to prove you have fulfilled all of the aims you set out to achieve. Therefore, while having more than one research aim is not necessarily disadvantageous, consider whether a single overarching one will do.
Research Objectives
Each of your research objectives should be SMART :
- Specific – is there any ambiguity in the action you are going to undertake, or is it focused and well-defined?
- Measurable – how will you measure progress and determine when you have achieved the action?
- Achievable – do you have the support, resources and facilities required to carry out the action?
- Relevant – is the action essential to the achievement of your research aim?
- Timebound – can you realistically complete the action in the available time alongside your other research tasks?
In addition to being SMART, your research objectives should start with a verb that helps communicate your intent. Common research verbs include:
Table of Research Verbs to Use in Aims and Objectives
| (Understanding and organising information) | (Solving problems using information) | (reaching conclusion from evidence) | (Breaking down into components) | (Judging merit) |
| Review Identify Explore Discover Discuss Summarise Describe | Interpret Apply Demonstrate Establish Determine Estimate Calculate Relate | Analyse Compare Inspect Examine Verify Select Test Arrange | Propose Design Formulate Collect Construct Prepare Undertake Assemble | Appraise Evaluate Compare Assess Recommend Conclude Select |
Last, format your objectives into a numbered list. This is because when you write your thesis or dissertation, you will at times need to make reference to a specific research objective; structuring your research objectives in a numbered list will provide a clear way of doing this.
To bring all this together, let’s compare the first research objective in the previous example with the above guidance:
Checking Research Objective Example Against Recommended Approach
Research Objective:
1. Develop finite element models using explicit dynamics to mimic mallet blows during cup/shell insertion, initially using simplified experimentally validated foam models to represent the acetabulum.
Checking Against Recommended Approach:
Q: Is it specific? A: Yes, it is clear what the student intends to do (produce a finite element model), why they intend to do it (mimic cup/shell blows) and their parameters have been well-defined ( using simplified experimentally validated foam models to represent the acetabulum ).
Q: Is it measurable? A: Yes, it is clear that the research objective will be achieved once the finite element model is complete.
Q: Is it achievable? A: Yes, provided the student has access to a computer lab, modelling software and laboratory data.
Q: Is it relevant? A: Yes, mimicking impacts to a cup/shell is fundamental to the overall aim of understanding how they deform when impacted upon.
Q: Is it timebound? A: Yes, it is possible to create a limited-scope finite element model in a relatively short time, especially if you already have experience in modelling.
Q: Does it start with a verb? A: Yes, it starts with ‘develop’, which makes the intent of the objective immediately clear.
Q: Is it a numbered list? A: Yes, it is the first research objective in a list of eight.
Mistakes in Writing Research Aims and Objectives
1. making your research aim too broad.
Having a research aim too broad becomes very difficult to achieve. Normally, this occurs when a student develops their research aim before they have a good understanding of what they want to research. Remember that at the end of your project and during your viva defence , you will have to prove that you have achieved your research aims; if they are too broad, this will be an almost impossible task. In the early stages of your research project, your priority should be to narrow your study to a specific area. A good way to do this is to take the time to study existing literature, question their current approaches, findings and limitations, and consider whether there are any recurring gaps that could be investigated .
Note: Achieving a set of aims does not necessarily mean proving or disproving a theory or hypothesis, even if your research aim was to, but having done enough work to provide a useful and original insight into the principles that underlie your research aim.
2. Making Your Research Objectives Too Ambitious
Be realistic about what you can achieve in the time you have available. It is natural to want to set ambitious research objectives that require sophisticated data collection and analysis, but only completing this with six months before the end of your PhD registration period is not a worthwhile trade-off.
3. Formulating Repetitive Research Objectives
Each research objective should have its own purpose and distinct measurable outcome. To this effect, a common mistake is to form research objectives which have large amounts of overlap. This makes it difficult to determine when an objective is truly complete, and also presents challenges in estimating the duration of objectives when creating your project timeline. It also makes it difficult to structure your thesis into unique chapters, making it more challenging for you to write and for your audience to read.
Fortunately, this oversight can be easily avoided by using SMART objectives.
Hopefully, you now have a good idea of how to create an effective set of aims and objectives for your research project, whether it be a thesis, dissertation or research paper. While it may be tempting to dive directly into your research, spending time on getting your aims and objectives right will give your research clear direction. This won’t only reduce the likelihood of problems arising later down the line, but will also lead to a more thorough and coherent research project.
Finding a PhD has never been this easy – search for a PhD by keyword, location or academic area of interest.
Browse PhDs Now
Join thousands of students.
Join thousands of other students and stay up to date with the latest PhD programmes, funding opportunities and advice.
- Thesis Action Plan New
- Academic Project Planner
Literature Navigator
Thesis dialogue blueprint, writing wizard's template, research proposal compass.
- Why students love us
- Rebels Blog
- Why we are different
- All Products
- Coming Soon
How to Align Research Questions and Objectives for a Successful Study

Aligning research questions and objectives is a critical step in conducting a successful study. This alignment ensures that the research remains focused, relevant, and methodologically sound. By clearly defining and interconnecting research questions and objectives, researchers can enhance the clarity, direction, and impact of their study.
Key Takeaways
- Understanding the relationship between research questions and objectives is fundamental for a coherent study design.
- Formulating clear and concise research questions helps in directing the research process effectively.
- Developing research objectives that align with research questions ensures that the study is focused and purposeful.
- A thorough literature review is essential for identifying research gaps and refining both questions and objectives.
- The iterative process of revisiting and refining research questions and objectives enhances the overall quality and alignment of the study.
Understanding the Relationship Between Research Questions and Objectives
Research questions and objectives are fundamental components of any research study. Understanding their relationship is crucial for ensuring the coherence and success of your research. Research questions are specific inquiries that guide your investigation, while research objectives are the goals you aim to achieve through your study. These elements are interdependent and must be aligned to provide a clear direction for your research.
Defining Research Questions
Research questions are the foundation of your study. They are specific, focused, and designed to address the core issues you wish to explore. Crafting effective research questions involves structured conversations: crafting effective interview protocols. identify objectives, define audience, determine key questions, design structure, create guide for focused and valuable insights. A well-formulated research question should be clear, concise, and researchable.
Defining Research Objectives
Research objectives are the specific goals that a researcher aims to achieve through their research study. These objectives are developed to guide the research process and provide a clear plan for how the research will be conducted, analyzed, and evaluated. They are broader than research questions and often encompass multiple aspects of the study. Maximizing resources: smart budgeting for successful research projects. key strategies include defining objectives, analyzing research questions, and budgeting for resources effectively.
Interdependence of Questions and Objectives
The relationship between research questions and objectives is inherently interdependent. Research questions help to narrow down the focus of the study, while research objectives provide a roadmap for achieving the desired outcomes. This interdependence ensures that the research remains focused and relevant, ultimately leading to more robust and impactful findings.
Formulating Clear and Concise Research Questions
Formulating clear and concise research questions is a critical step in the research process. A well-crafted research question serves as the foundation for your study, guiding your methodology and analysis. A strong research question goes beyond mere inquiry; it embodies a set of distinct qualities that elevate it from the realm of casual pondering to that of rigorous academic investigation.
Developing Research Objectives Aligned with Research Questions
Steps to define research objectives.
To define research objectives, start by clearly understanding your research questions . This involves breaking down the questions into specific, actionable goals. Ensure each objective is directly related to a research question to maintain alignment. Follow these steps:
- Identify the main research question.
- Break it down into sub-questions if necessary.
- Translate each question into a specific objective.
- Ensure the objectives are clear and concise.
- Review and refine the objectives to ensure they are achievable.
Ensuring Measurability and Achievability
When developing research objectives, it is crucial to ensure they are both measurable and achievable. This means setting objectives that can be quantified and realistically accomplished within the scope of your study. Use the SMART criteria (Specific, Measurable, Achievable, Relevant, Time-bound) to evaluate your objectives. For example, instead of stating an objective as "improve understanding of a topic," specify it as "increase the number of correct responses on a topic-related quiz by 20%."
Examples of Aligned Objectives
To illustrate the alignment between research questions and objectives, consider the following examples:
- Objective: Identify and analyze the key factors affecting student performance in online learning environments.
- Objective: Examine the correlation between social media usage patterns and mental health indicators among teenagers.
By following these guidelines, you can ensure that your research objectives are well-aligned with your research questions, leading to a more focused and successful study.
The Role of Literature Review in Aligning Research Questions and Objectives
A literature review is a comprehensive summary and analysis of the existing research on a particular topic. It serves several critical purposes in the research process. Conducting a thorough literature review can help you understand what research has been done in the area and what gaps exist in the literature. This understanding is crucial for aligning your research questions and objectives effectively.
Identifying Research Gaps
When you conduct a literature review, you are essentially mapping out the existing knowledge landscape. This helps in identifying gaps where further research is needed. Recognizing these gaps allows you to formulate research questions that address unexplored areas, thereby making your study more relevant and impactful.
Supporting Objectives with Literature
The literature review not only helps in formulating research questions but also in supporting your research objectives. By reviewing relevant literature, you can find evidence and theoretical backing for your objectives, ensuring they are grounded in existing research. This step is essential for the credibility and validity of your study.
Refining Questions Based on Literature
As you delve deeper into the literature, you may find that your initial research questions need refinement. The insights gained from the literature can help you tweak your questions to be more precise and aligned with your objectives. This iterative process ensures that your research questions are both relevant and feasible.
In summary, the literature review is an indispensable tool in the research process. It aids in identifying research gaps, supports your objectives with existing knowledge, and helps refine your research questions. Utilizing resources like the Literature Navigator can streamline this process, making it easier to find literature and align your study components effectively.
Iterative Process of Aligning Research Questions and Objectives
The process of aligning research questions and objectives is inherently iterative. This means that you will need to revisit and refine your research questions and objectives multiple times throughout your study. This iterative approach ensures that your research remains focused and relevant.
Ensuring Methodological Consistency with Research Questions and Objectives
Ensuring methodological consistency is crucial for the success of your research study. Consistency in the title, problem, purpose, and research question improves the logic and transparency of your research. When these components are aligned, research design and planning become more coherent, and research reports are more readable. This alignment is an important issue in a research project because one's research questions are derived from the research objective. Research questions further distill the objective by more clearly focusing the research objective, and the purpose provides clues to the type of research design.
Evaluating the Alignment of Research Questions and Objectives
Evaluating the alignment of research questions and objectives is a critical step in ensuring the success of your study. This process involves a thorough examination of how well your research questions reflect and support your objectives. Crafting a well-aligned thesis statement is crucial in academic writing. Regularly refine it to guide readers and maintain coherence with research goals.
Evaluating the alignment of research questions and objectives is crucial for the success of any academic project. Ensuring that your research questions are well-aligned with your objectives can significantly enhance the clarity and focus of your study. If you're struggling with this aspect of your thesis, our step-by-step Thesis Action Plan can guide you through the process. Visit our website to learn more and claim your special offer now !
In conclusion, the alignment of research questions and objectives is a critical aspect of conducting a successful study. This alignment ensures that the research is focused, coherent, and methodologically sound. By clearly defining research objectives and formulating research questions that directly address these objectives, researchers can maintain a clear direction throughout their study. This process not only enhances the relevance and impact of the research but also facilitates the development of a robust research design. As such, meticulous attention to aligning research questions with objectives is indispensable for producing high-quality, meaningful, and impactful research outcomes.
Frequently Asked Questions
What is the difference between a research question and a research objective.
A research question is a specific query the study aims to answer, while a research objective outlines the goals the research intends to achieve. Research questions guide the focus of the study, and objectives provide a roadmap for achieving the desired outcomes.
How do I formulate effective research questions?
Effective research questions should be clear, focused, and researchable. They should address a specific problem, be feasible to answer within the scope of the study, and be significant to the field of research.
Why is it important to align research questions with research objectives?
Aligning research questions with research objectives ensures that the study remains focused and coherent. This alignment helps in systematically addressing the research problem and achieving the desired outcomes, leading to a successful study.
Can you provide an example of a well-formulated research question and its aligned objective?
Sure! Example: Research Question: 'What are the effects of remote work on employee productivity?' Aligned Objective: 'To assess the impact of remote work on employee productivity levels in various industries.'
How does a literature review help in aligning research questions and objectives?
A literature review helps identify existing research gaps and supports the formulation of research objectives. It provides a theoretical foundation for refining research questions and ensures that the study is grounded in existing knowledge.
What are common pitfalls to avoid when aligning research questions and objectives?
Common pitfalls include formulating vague or overly broad questions, setting unrealistic objectives, and failing to ensure that the questions and objectives are researchable and relevant. It's important to be precise, realistic, and ensure a clear connection between the two.

Discovering Statistics Using IBM SPSS Statistics: A Fun and Informative Guide

Unlocking the Power of Data: A Review of 'Essentials of Modern Business Statistics with Microsoft Excel'

Discovering Statistics Using SAS: A Comprehensive Review

How to Deal with a Total Lack of Motivation, Stress, and Anxiety When Finishing Your Master's Thesis

Mastering the First Step: How to Start Your Thesis with Confidence

Thesis Revision Made Simple: Techniques for Perfecting Your Academic Work

Thesis Action Plan

Integrating Calm into Your Study Routine: The Power of Mindfulness in Education
How to determine the perfect research proposal length.
- Blog Articles
- Affiliate Program
- Terms and Conditions
- Payment and Shipping Terms
- Privacy Policy
- Return Policy
© 2024 Research Rebels, All rights reserved.
Your cart is currently empty.
Difference between Research Questions and Research Objectives
When embarking on a research project, it’s important to have a clear understanding of the distinction between research questions and research objectives. Both are key components of a research study, but they differ in their focus and purpose.
The main difference is that research questions focus on the general purpose or aim of the study whereas research objectives provide specific, measurable, and attainable steps to achieve the research questions.
Before we move to the differences, let’s understand what are Research Questions and Research Objectives:

Now, let’s move to Research Questions vs Research Objectives:
Major differences between Research Questions and Research Objectives
| Research Questions | Research Objectives |
|---|---|
| Research questions focus on the main topic or issue being investigated. | Research objectives focus on the specific steps the researcher will take to answer those questions. |
| Research questions can sometimes be vague or open-ended. | Research objectives must be clear, specific and measurable. |
| Research questions are general in nature and aim to cover a broad aspect of the topic being researched. | Research objectives are specific and cover limited aspects of the topic. |
| Research questions might change and be formed as the research progresses. | Research objectives are usually set before the commencement of a research work and may not change as the research progresses. |
| Research questions are used to guide the overall direction of the study. | Research objectives provide specific steps to achieve the research questions. |
Note that sometimes, the question might also be asked as “distinguish between Research Questions and Research Objectives”.
Final words
Research questions and research objectives are related, they are not interchangeable terms. Research questions describe the goals or aims of a study in a broader sense, while research objectives provide specific, measurable, achievable steps to achieve those goals.
Understanding the difference between these two terms can help you design and execute a more effective research study.
You can view other “differences between” posts by clicking here .
If you have a related query, feel free to let us know in the comments below.
Also, kindly share the information with your friends who you think might be interested in reading it.
Leave a Reply Cancel reply
Save my name, email, and website in this browser for the next time I comment.
- Call: +254725788400
- [email protected]
1.3 Research Objectives and Research Questions
By Anthony M. Wanjohi
A good research problem is that which generates a number of other research questions or objectives. After stating the research problem, you should go ahead to generated research questions or objectives. You may choose to use either research questions or objectives especially if they are referring to one and the same phenomenon.
Research questions refer to questions, which the researcher would like to be answered by carrying out the proposed study. The only difference between research questions and objectives is that research questions are stated in a question form while objectives are stated in a statement form. For an objective to be good, it should be SMART: Specific, Measurable, Achievable, Relevant and Time-bound.
The importance of research objectives lies in the fact that they determine:
- The kind of questions to be asked. In other words, research questions are derived from the objectives.
- The data collection and analysis procedure to be used. Data collection tools are developed from the research objectives.
- The design of the proposed study. Various research designs have different research objectives.
Using the study on Teacher and Parental Factors Affecting Students’ Academic Performance in Private Secondary Schools in Embu Municipality, Kenya as an example, you may state your research specific research objectives as follows:
- To find out the teacher factors influencing the students’ academic performance in private secondary schools in Embu Municipality?
- To find out the parental factors influencing the students’ academic performance in private secondary schools in Embu Municipality?
- To determine the extent to which teacher/parental factors affect the students’ academic performance in private secondary schools in Embu Municipality
- To find out what measures can be put in place to improve the students’ academic performance in private secondary schools in Embu Municipality
Research Questions:
From the aforementioned research objectives, the following research questions can be stated:
- What are the teachers factors influencing the students’ academic performance in private secondary schools in Embu Municipality?
- What are the parental factors influencing the students’ academic performance in private secondary Schools in Embu Municipality?
- To what extent do teacher/parental factors affect the students’ academic performance in private secondary Schools in Embu Municipality?
- What measures can be put in place to improve students’ academic performance in private secondary schools in Embu Municipality?
Note that you can choose to use either research objectives or the research questions if they are the same as it is in the given examples. But in the situation where you derive two or more research questions from one objective, you can use both research objectives and research questions in your proposed study. Read more…
Suggested Citation (APA):
Wanjohi, A.M. (2012). Research objectives and research questions. Retrieved online from at www.kenpro.org/research-objectives-and-research-questions

About KENPRO
Kenya Projects Organization is a membership organization founded and registered in Kenya in the year 2009. The main objective of the organization is to build individual and institutional capacities through project planning and management, research, publishing and IT.
Related Posts
KENPRO strengthens human and institutional capacities through providing best practices in project management, research and IT solutions, with a component of training.
Related Sites
- African Journal of Education and Social Sciences
- AfroKid Computing
- Afri Digital Marketing
- Higher Institute of Applied Learning
- Schools Net Kenya
- School Study Resources
- Writers Bureau Centre
Recent Publications
Innovative application of solar and biogas in agriculture in kenya, 6 ways to attract high-quality talent to your business, uganda solar installation capacity growth trends between 2012 and 2022, kenya solar installation capacity growth trends between 2012 and 2022, an overview of solar energy growth trends from 2012 to 2022 in the context of africa and kenya, why manager-employee relations are crucial for companies, subscription.
Subscribe below to receive updates on our publications
- +254 734 579 299
- +254 725 788 400
- General Inquiries: [email protected]
St. Marks Academy Admin Block, Off Magadi Road, P.O. Box 15509-00503, Mbagathi, Nairobi-Kenya
Kenya Projects Organization (KENPRO) is a registered membership organization in Kenya (Reg. No. KJD/N/CBO/1800168/13)
Stack Exchange Network
Stack Exchange network consists of 183 Q&A communities including Stack Overflow , the largest, most trusted online community for developers to learn, share their knowledge, and build their careers.
Q&A for work
Connect and share knowledge within a single location that is structured and easy to search.
Difference between research question and research objective
What is the difference between research question and research objective?
In my opinion, every research question can be paraphrased as a research objective and vice versa. Am I right?
- terminology
- research-proposal
- The question is what will be answered, the objectives might be what could follow from the answers (which justifies the need to answer the question). – user2768 Commented Nov 30, 2017 at 12:31
- 1 Welcome to Academia SE. You’ll probably get a more helpful answer if you specify why you wish to know this. – Wrzlprmft ♦ Commented Nov 30, 2017 at 13:50
Although the specific formal definition can be field specific, Farrugia et al do a nice job of laying out "research questions", "hypotheses", and "objectives" in their open access article (linked above). Note their article targets medical researchers, but applies to other fields as well.
To summarize/highlight their definitions:
- Research questions "arise out of a perceived knowledge deficit within a subject area or field of study." These may be answered either using literature reviews or primary research.
- Research hypothesis are the formal ideas one seeks to test. (The linked article focuses on null hypothesis test, Chamberlin (reprinted in Science 1965, first published in Science in the late-1800s) ) does a better job of explaining hypotheses. Chamberlin advocates for multiple working hypotheses where you have multiple competing ideas.,
- Research objectives "should be coupled with the hypothesis of the study". These are what the study specifically seeks to do. (e.g., what is to be measured to test a hypothesis?).
- 1 One may add that there's not always a specific formal definition, simply because it's not necessary to have one. Science primarily seeks to advance knowledge, and the meta-terminology for describing a knowledge advancement can vary. – lighthouse keeper Commented Nov 30, 2017 at 17:14
You must log in to answer this question.
Not the answer you're looking for browse other questions tagged terminology research-proposal ..
- Featured on Meta
- Bringing clarity to status tag usage on meta sites
- We've made changes to our Terms of Service & Privacy Policy - July 2024
- Announcing a change to the data-dump process
Hot Network Questions
- Why does flow separation cause an increase in pressure drag?
- Encode a VarInt
- My supervisor wants me to switch to another software/programming language that I am not proficient in. What to do?
- Is this a mistake or am I misunderstanding how to calculate a capacitor's impedance with ESR and ESL?
- Where to donate foreign-language academic books?
- Is there a way to resist spells or abilities with an AOE coming from my teammates, or exclude certain beings from the effect?
- Dutch Public Transportation Electronic Payment Options
- Large file manipulation
- If inflation/cost of living is such a complex difficult problem, then why has the price of drugs been absoultly perfectly stable my whole life?
- Are the any polls on the opinion about Hamas in the broader Arab or Muslim world?
- Planning to rebuild detached storage room (in the US)
- Why does a halfing's racial trait lucky specify you must use the next roll?
- Fast matrix multiplication for large matrices in Python
- Do metal objects attract lightning?
- How is it possible to know a proposed perpetual motion machine won't work without even looking at it?
- Slicing Graph by path
- If a trigger runs an update will it ALWAYS have the same timestamp for a temporal table?
- What happens if all nine Supreme Justices recuse themselves?
- I am a sailor. I am planning to call my family onboard with me on the ship from the suez
- How could I contact the Betriebsrat (Workers' Union) of my employer behind his back?
- Background for the Elkies-Klagsbrun curve of rank 29
- Stuck on Sokoban
- Historical U.S. political party "realignments"?
- Cramer's Rule when the determinant of coefficient matrix is zero?
Ohio State nav bar
The Ohio State University
- BuckeyeLink
- Find People
- Search Ohio State
Research Questions & Hypotheses
Generally, in quantitative studies, reviewers expect hypotheses rather than research questions. However, both research questions and hypotheses serve different purposes and can be beneficial when used together.
Research Questions
Clarify the research’s aim (farrugia et al., 2010).
- Research often begins with an interest in a topic, but a deep understanding of the subject is crucial to formulate an appropriate research question.
- Descriptive: “What factors most influence the academic achievement of senior high school students?”
- Comparative: “What is the performance difference between teaching methods A and B?”
- Relationship-based: “What is the relationship between self-efficacy and academic achievement?”
- Increasing knowledge about a subject can be achieved through systematic literature reviews, in-depth interviews with patients (and proxies), focus groups, and consultations with field experts.
- Some funding bodies, like the Canadian Institute for Health Research, recommend conducting a systematic review or a pilot study before seeking grants for full trials.
- The presence of multiple research questions in a study can complicate the design, statistical analysis, and feasibility.
- It’s advisable to focus on a single primary research question for the study.
- The primary question, clearly stated at the end of a grant proposal’s introduction, usually specifies the study population, intervention, and other relevant factors.
- The FINER criteria underscore aspects that can enhance the chances of a successful research project, including specifying the population of interest, aligning with scientific and public interest, clinical relevance, and contribution to the field, while complying with ethical and national research standards.
| Feasible | ||
| Interesting | ||
| Novel | ||
| Ethical | ||
| Relevant |
- The P ICOT approach is crucial in developing the study’s framework and protocol, influencing inclusion and exclusion criteria and identifying patient groups for inclusion.
| Population (patients) | ||
| Intervention (for intervention studies only) | ||
| Comparison group | ||
| Outcome of interest | ||
| Time |
- Defining the specific population, intervention, comparator, and outcome helps in selecting the right outcome measurement tool.
- The more precise the population definition and stricter the inclusion and exclusion criteria, the more significant the impact on the interpretation, applicability, and generalizability of the research findings.
- A restricted study population enhances internal validity but may limit the study’s external validity and generalizability to clinical practice.
- A broadly defined study population may better reflect clinical practice but could increase bias and reduce internal validity.
- An inadequately formulated research question can negatively impact study design, potentially leading to ineffective outcomes and affecting publication prospects.
Checklist: Good research questions for social science projects (Panke, 2018)
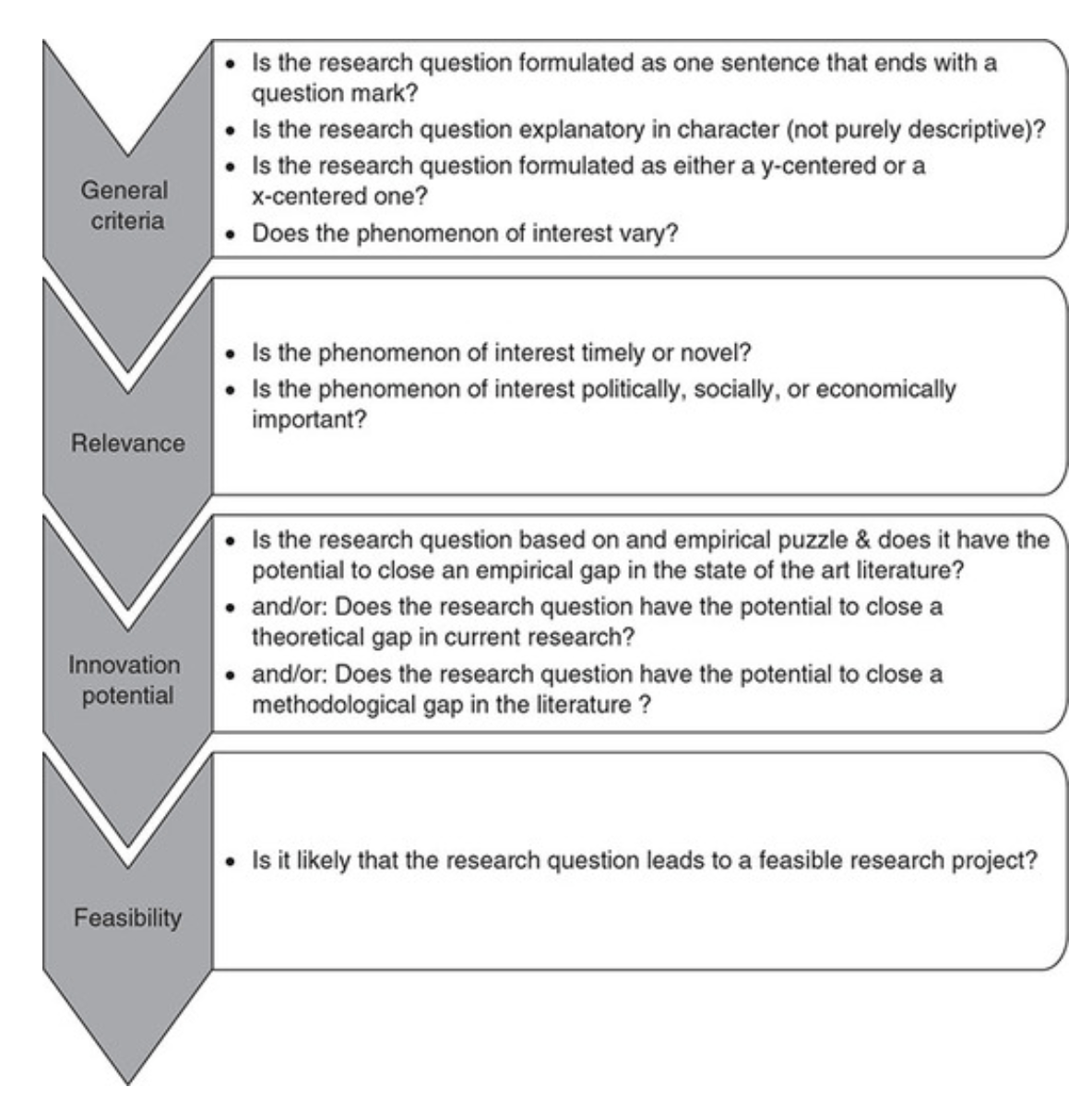
Research Hypotheses
Present the researcher’s predictions based on specific statements.
- These statements define the research problem or issue and indicate the direction of the researcher’s predictions.
- Formulating the research question and hypothesis from existing data (e.g., a database) can lead to multiple statistical comparisons and potentially spurious findings due to chance.
- The research or clinical hypothesis, derived from the research question, shapes the study’s key elements: sampling strategy, intervention, comparison, and outcome variables.
- Hypotheses can express a single outcome or multiple outcomes.
- After statistical testing, the null hypothesis is either rejected or not rejected based on whether the study’s findings are statistically significant.
- Hypothesis testing helps determine if observed findings are due to true differences and not chance.
- Hypotheses can be 1-sided (specific direction of difference) or 2-sided (presence of a difference without specifying direction).
- 2-sided hypotheses are generally preferred unless there’s a strong justification for a 1-sided hypothesis.
- A solid research hypothesis, informed by a good research question, influences the research design and paves the way for defining clear research objectives.
Types of Research Hypothesis
- In a Y-centered research design, the focus is on the dependent variable (DV) which is specified in the research question. Theories are then used to identify independent variables (IV) and explain their causal relationship with the DV.
- Example: “An increase in teacher-led instructional time (IV) is likely to improve student reading comprehension scores (DV), because extensive guided practice under expert supervision enhances learning retention and skill mastery.”
- Hypothesis Explanation: The dependent variable (student reading comprehension scores) is the focus, and the hypothesis explores how changes in the independent variable (teacher-led instructional time) affect it.
- In X-centered research designs, the independent variable is specified in the research question. Theories are used to determine potential dependent variables and the causal mechanisms at play.
- Example: “Implementing technology-based learning tools (IV) is likely to enhance student engagement in the classroom (DV), because interactive and multimedia content increases student interest and participation.”
- Hypothesis Explanation: The independent variable (technology-based learning tools) is the focus, with the hypothesis exploring its impact on a potential dependent variable (student engagement).
- Probabilistic hypotheses suggest that changes in the independent variable are likely to lead to changes in the dependent variable in a predictable manner, but not with absolute certainty.
- Example: “The more teachers engage in professional development programs (IV), the more their teaching effectiveness (DV) is likely to improve, because continuous training updates pedagogical skills and knowledge.”
- Hypothesis Explanation: This hypothesis implies a probable relationship between the extent of professional development (IV) and teaching effectiveness (DV).
- Deterministic hypotheses state that a specific change in the independent variable will lead to a specific change in the dependent variable, implying a more direct and certain relationship.
- Example: “If the school curriculum changes from traditional lecture-based methods to project-based learning (IV), then student collaboration skills (DV) are expected to improve because project-based learning inherently requires teamwork and peer interaction.”
- Hypothesis Explanation: This hypothesis presumes a direct and definite outcome (improvement in collaboration skills) resulting from a specific change in the teaching method.
- Example : “Students who identify as visual learners will score higher on tests that are presented in a visually rich format compared to tests presented in a text-only format.”
- Explanation : This hypothesis aims to describe the potential difference in test scores between visual learners taking visually rich tests and text-only tests, without implying a direct cause-and-effect relationship.
- Example : “Teaching method A will improve student performance more than method B.”
- Explanation : This hypothesis compares the effectiveness of two different teaching methods, suggesting that one will lead to better student performance than the other. It implies a direct comparison but does not necessarily establish a causal mechanism.
- Example : “Students with higher self-efficacy will show higher levels of academic achievement.”
- Explanation : This hypothesis predicts a relationship between the variable of self-efficacy and academic achievement. Unlike a causal hypothesis, it does not necessarily suggest that one variable causes changes in the other, but rather that they are related in some way.
Tips for developing research questions and hypotheses for research studies
- Perform a systematic literature review (if one has not been done) to increase knowledge and familiarity with the topic and to assist with research development.
- Learn about current trends and technological advances on the topic.
- Seek careful input from experts, mentors, colleagues, and collaborators to refine your research question as this will aid in developing the research question and guide the research study.
- Use the FINER criteria in the development of the research question.
- Ensure that the research question follows PICOT format.
- Develop a research hypothesis from the research question.
- Ensure that the research question and objectives are answerable, feasible, and clinically relevant.
If your research hypotheses are derived from your research questions, particularly when multiple hypotheses address a single question, it’s recommended to use both research questions and hypotheses. However, if this isn’t the case, using hypotheses over research questions is advised. It’s important to note these are general guidelines, not strict rules. If you opt not to use hypotheses, consult with your supervisor for the best approach.
Farrugia, P., Petrisor, B. A., Farrokhyar, F., & Bhandari, M. (2010). Practical tips for surgical research: Research questions, hypotheses and objectives. Canadian journal of surgery. Journal canadien de chirurgie , 53 (4), 278–281.
Hulley, S. B., Cummings, S. R., Browner, W. S., Grady, D., & Newman, T. B. (2007). Designing clinical research. Philadelphia.
Panke, D. (2018). Research design & method selection: Making good choices in the social sciences. Research Design & Method Selection , 1-368.

Formulating Research Aims and Objectives
Formulating research aim and objectives in an appropriate manner is one of the most important aspects of your thesis. This is because research aim and objectives determine the scope, depth and the overall direction of the research. Research question is the central question of the study that has to be answered on the basis of research findings.
Research aim emphasizes what needs to be achieved within the scope of the research, by the end of the research process. Achievement of research aim provides answer to the research question.
Research objectives divide research aim into several parts and address each part separately. Research aim specifies WHAT needs to be studied and research objectives comprise a number of steps that address HOW research aim will be achieved.
As a rule of dumb, there would be one research aim and several research objectives. Achievement of each research objective will lead to the achievement of the research aim.
Consider the following as an example:
Research title: Effects of organizational culture on business profitability: a case study of Virgin Atlantic
Research aim: To assess the effects of Virgin Atlantic organizational culture on business profitability
Following research objectives would facilitate the achievement of this aim:
- Analyzing the nature of organizational culture at Virgin Atlantic by September 1, 2022
- Identifying factors impacting Virgin Atlantic organizational culture by September 16, 2022
- Analyzing impacts of Virgin Atlantic organizational culture on employee performances by September 30, 2022
- Providing recommendations to Virgin Atlantic strategic level management in terms of increasing the level of effectiveness of organizational culture by October 5, 2022
Figure below illustrates additional examples in formulating research aims and objectives:

Formulation of research question, aim and objectives
Common mistakes in the formulation of research aim relate to the following:
1. Choosing the topic too broadly . This is the most common mistake. For example, a research title of “an analysis of leadership practices” can be classified as too broad because the title fails to answer the following questions:
a) Which aspects of leadership practices? Leadership has many aspects such as employee motivation, ethical behaviour, strategic planning, change management etc. An attempt to cover all of these aspects of organizational leadership within a single research will result in an unfocused and poor work.
b) An analysis of leadership practices in which country? Leadership practices tend to be different in various countries due to cross-cultural differences, legislations and a range of other region-specific factors. Therefore, a study of leadership practices needs to be country-specific.
c) Analysis of leadership practices in which company or industry? Similar to the point above, analysis of leadership practices needs to take into account industry-specific and/or company-specific differences, and there is no way to conduct a leadership research that relates to all industries and organizations in an equal manner.
Accordingly, as an example “a study into the impacts of ethical behaviour of a leader on the level of employee motivation in US healthcare sector” would be a more appropriate title than simply “An analysis of leadership practices”.
2. Setting an unrealistic aim . Formulation of a research aim that involves in-depth interviews with Apple strategic level management by an undergraduate level student can be specified as a bit over-ambitious. This is because securing an interview with Apple CEO Tim Cook or members of Apple Board of Directors might not be easy. This is an extreme example of course, but you got the idea. Instead, you may aim to interview the manager of your local Apple store and adopt a more feasible strategy to get your dissertation completed.
3. Choosing research methods incompatible with the timeframe available . Conducting interviews with 20 sample group members and collecting primary data through 2 focus groups when only three months left until submission of your dissertation can be very difficult, if not impossible. Accordingly, timeframe available need to be taken into account when formulating research aims and objectives and selecting research methods.
Moreover, research objectives need to be formulated according to SMART principle,
where the abbreviation stands for specific, measurable, achievable, realistic, and time-bound.
| Study employee motivation of Coca-Cola | To study the impacts of management practices on the levels of employee motivation at Coca-Cola US by December 5, 2022
|
| Analyze consumer behaviour in catering industry
| Analyzing changes in consumer behaviour in catering industry in the 21 century in the UK by March 1, 2022 |
| Recommend Toyota Motor Corporation management on new market entry strategy
| Formulating recommendations to Toyota Motor Corporation management on the choice of appropriate strategy to enter Vietnam market by June 9, 2022
|
| Analyze the impact of social media marketing on business
| Assessing impacts of integration of social media into marketing strategy on the level of brand awareness by March 30, 2022
|
| Finding out about time management principles used by Accenture managers | Identifying main time-management strategies used by managers of Accenture France by December 1, 2022 |
Examples of SMART research objectives
At the conclusion part of your research project you will need to reflect on the level of achievement of research aims and objectives. In case your research aims and objectives are not fully achieved by the end of the study, you will need to discuss the reasons. These may include initial inappropriate formulation of research aims and objectives, effects of other variables that were not considered at the beginning of the research or changes in some circumstances during the research process.

John Dudovskiy
Frequently asked questions
What’s the difference between research aims and objectives.
A research aim is a broad statement indicating the general purpose of your research project. It should appear in your introduction at the end of your problem statement , before your research objectives.
Research objectives are more specific than your research aim. They indicate the specific ways you’ll address the overarching aim.
Frequently asked questions: Writing a research paper
A research project is an academic, scientific, or professional undertaking to answer a research question . Research projects can take many forms, such as qualitative or quantitative , descriptive , longitudinal , experimental , or correlational . What kind of research approach you choose will depend on your topic.
The best way to remember the difference between a research plan and a research proposal is that they have fundamentally different audiences. A research plan helps you, the researcher, organize your thoughts. On the other hand, a dissertation proposal or research proposal aims to convince others (e.g., a supervisor, a funding body, or a dissertation committee) that your research topic is relevant and worthy of being conducted.
Formulating a main research question can be a difficult task. Overall, your question should contribute to solving the problem that you have defined in your problem statement .
However, it should also fulfill criteria in three main areas:
- Researchability
- Feasibility and specificity
- Relevance and originality
Research questions anchor your whole project, so it’s important to spend some time refining them.
In general, they should be:
- Focused and researchable
- Answerable using credible sources
- Complex and arguable
- Feasible and specific
- Relevant and original
All research questions should be:
- Focused on a single problem or issue
- Researchable using primary and/or secondary sources
- Feasible to answer within the timeframe and practical constraints
- Specific enough to answer thoroughly
- Complex enough to develop the answer over the space of a paper or thesis
- Relevant to your field of study and/or society more broadly

Once you’ve decided on your research objectives , you need to explain them in your paper, at the end of your problem statement .
Keep your research objectives clear and concise, and use appropriate verbs to accurately convey the work that you will carry out for each one.
I will compare …
Your research objectives indicate how you’ll try to address your research problem and should be specific:
Research objectives describe what you intend your research project to accomplish.
They summarize the approach and purpose of the project and help to focus your research.
Your objectives should appear in the introduction of your research paper , at the end of your problem statement .
The main guidelines for formatting a paper in Chicago style are to:
- Use a standard font like 12 pt Times New Roman
- Use 1 inch margins or larger
- Apply double line spacing
- Indent every new paragraph ½ inch
- Include a title page
- Place page numbers in the top right or bottom center
- Cite your sources with author-date citations or Chicago footnotes
- Include a bibliography or reference list
To automatically generate accurate Chicago references, you can use Scribbr’s free Chicago reference generator .
The main guidelines for formatting a paper in MLA style are as follows:
- Use an easily readable font like 12 pt Times New Roman
- Set 1 inch page margins
- Include a four-line MLA heading on the first page
- Center the paper’s title
- Use title case capitalization for headings
- Cite your sources with MLA in-text citations
- List all sources cited on a Works Cited page at the end
To format a paper in APA Style , follow these guidelines:
- Use a standard font like 12 pt Times New Roman or 11 pt Arial
- If submitting for publication, insert a running head on every page
- Apply APA heading styles
- Cite your sources with APA in-text citations
- List all sources cited on a reference page at the end
No, it’s not appropriate to present new arguments or evidence in the conclusion . While you might be tempted to save a striking argument for last, research papers follow a more formal structure than this.
All your findings and arguments should be presented in the body of the text (more specifically in the results and discussion sections if you are following a scientific structure). The conclusion is meant to summarize and reflect on the evidence and arguments you have already presented, not introduce new ones.
The conclusion of a research paper has several key elements you should make sure to include:
- A restatement of the research problem
- A summary of your key arguments and/or findings
- A short discussion of the implications of your research
Don’t feel that you have to write the introduction first. The introduction is often one of the last parts of the research paper you’ll write, along with the conclusion.
This is because it can be easier to introduce your paper once you’ve already written the body ; you may not have the clearest idea of your arguments until you’ve written them, and things can change during the writing process .
The way you present your research problem in your introduction varies depending on the nature of your research paper . A research paper that presents a sustained argument will usually encapsulate this argument in a thesis statement .
A research paper designed to present the results of empirical research tends to present a research question that it seeks to answer. It may also include a hypothesis —a prediction that will be confirmed or disproved by your research.
The introduction of a research paper includes several key elements:
- A hook to catch the reader’s interest
- Relevant background on the topic
- Details of your research problem
and your problem statement
- A thesis statement or research question
- Sometimes an overview of the paper
Ask our team
Want to contact us directly? No problem. We are always here for you.
- Email [email protected]
- Start live chat
- Call +1 (510) 822-8066
- WhatsApp +31 20 261 6040

Our team helps students graduate by offering:
- A world-class citation generator
- Plagiarism Checker software powered by Turnitin
- Innovative Citation Checker software
- Professional proofreading services
- Over 300 helpful articles about academic writing, citing sources, plagiarism, and more
Scribbr specializes in editing study-related documents . We proofread:
- PhD dissertations
- Research proposals
- Personal statements
- Admission essays
- Motivation letters
- Reflection papers
- Journal articles
- Capstone projects
Scribbr’s Plagiarism Checker is powered by elements of Turnitin’s Similarity Checker , namely the plagiarism detection software and the Internet Archive and Premium Scholarly Publications content databases .
The add-on AI detector is powered by Scribbr’s proprietary software.
The Scribbr Citation Generator is developed using the open-source Citation Style Language (CSL) project and Frank Bennett’s citeproc-js . It’s the same technology used by dozens of other popular citation tools, including Mendeley and Zotero.
You can find all the citation styles and locales used in the Scribbr Citation Generator in our publicly accessible repository on Github .
Research Problem vs. Research Question
What's the difference.
Research problem and research question are two essential components of any research study. The research problem refers to the issue or gap in knowledge that the researcher aims to address through their study. It identifies the area of research that requires further investigation and highlights the significance of the study. On the other hand, the research question is a specific inquiry that the researcher formulates to guide their investigation. It is a concise and focused query that helps to narrow down the research problem and provides a clear direction for the study. While the research problem sets the broader context, the research question provides a specific and measurable objective for the research study.
| Attribute | Research Problem | Research Question |
|---|---|---|
| Definition | A statement that identifies an area of concern or knowledge gap to be addressed through research. | An interrogative statement that seeks to explore or investigate a specific aspect of the research problem. |
| Focus | Identifies the broader issue or topic that needs to be studied. | Specifically targets a particular aspect or dimension of the research problem. |
| Scope | Can be broad and encompass multiple sub-issues or dimensions. | Usually narrower in scope, focusing on a specific aspect or relationship. |
| Format | Typically presented as a declarative statement. | Presented as an interrogative sentence. |
| Role | Forms the basis for the research study and guides the entire research process. | Provides a specific direction for the research study and helps in generating hypotheses. |
| Complexity | Can be complex and multifaceted, involving various factors and variables. | Can be relatively simpler, focusing on a specific aspect or relationship. |
Further Detail
Introduction.
Research is a systematic process that involves the exploration and investigation of a particular topic or issue. It aims to generate new knowledge, solve problems, or answer specific questions. In any research endeavor, it is crucial to clearly define the research problem and research question. While they are closely related, they have distinct attributes that shape the research process. This article will delve into the characteristics of research problems and research questions, highlighting their similarities and differences.
Research Problem
A research problem is the foundation of any research study. It refers to an area of concern or a gap in knowledge that requires investigation. Identifying a research problem is the initial step in the research process, as it sets the direction and purpose of the study. A research problem should be specific, clear, and well-defined to guide the research process effectively.
One of the key attributes of a research problem is that it should be significant. It should address an issue that has practical or theoretical implications and contributes to the existing body of knowledge. A significant research problem has the potential to make a positive impact on society, industry, or academia.
Furthermore, a research problem should be researchable. This means that it should be feasible to investigate and gather relevant data to address the problem. It should be within the researcher's capabilities and resources to conduct the study. A research problem that is too broad or vague may hinder the research process and lead to inconclusive results.
Additionally, a research problem should be specific and well-defined. It should clearly state the variables or concepts under investigation and provide a clear focus for the study. A well-defined research problem helps in formulating research questions and hypotheses, as it narrows down the scope of the study.
Lastly, a research problem should be original. It should contribute to the existing body of knowledge by addressing a gap or extending previous research. Originality ensures that the research study adds value and novelty to the field, making it relevant and interesting to researchers and practitioners.
Research Question
A research question is a specific inquiry that guides the research process and aims to provide an answer or solution to the research problem. It is derived from the research problem and helps in focusing the study, collecting relevant data, and analyzing the findings. A well-formulated research question is crucial for conducting a successful research study.
Similar to a research problem, a research question should be clear and specific. It should be concise and focused on a particular aspect of the research problem. A clear research question helps in determining the appropriate research design, methodology, and data collection techniques.
Furthermore, a research question should be answerable. It should be feasible to gather data and evidence to address the research question. An answerable research question ensures that the research study is practical and achievable within the given constraints.
A research question should also be relevant. It should directly relate to the research problem and contribute to the existing body of knowledge. A relevant research question ensures that the study has significance and value in the field, making it meaningful to researchers and stakeholders.
Lastly, a research question should be specific to the research context. It should consider the scope, objectives, and limitations of the study. A specific research question helps in avoiding ambiguity and ensures that the research study remains focused and coherent.
While research problems and research questions share some similarities, they also have distinct attributes that differentiate them. Both research problems and research questions should be clear, specific, and relevant to the research study. They should address a gap in knowledge and contribute to the existing body of knowledge.
However, a research problem is broader in scope compared to a research question. It sets the overall direction and purpose of the study, while a research question focuses on a specific aspect or inquiry within the research problem. A research problem provides a broader context for the study, while a research question narrows down the focus and guides the investigation.
Another difference lies in their formulation. A research problem is typically formulated as a statement or a declarative sentence, highlighting the area of concern or gap in knowledge. On the other hand, a research question is formulated as an interrogative sentence, posing a specific inquiry that needs to be answered or explored.
Furthermore, a research problem is often derived from a literature review or an analysis of existing research. It identifies the gap or area of concern based on the current state of knowledge. On the contrary, a research question is derived from the research problem itself. It is formulated to address the specific aspect or inquiry identified in the research problem.
Lastly, a research problem is usually stated at the beginning of a research study, while research questions are developed during the research design phase. The research problem sets the foundation for the study, while research questions are refined and finalized based on the research problem and objectives.
In conclusion, research problems and research questions are essential components of any research study. While they share similarities in terms of being clear, specific, and relevant, they also have distinct attributes that shape the research process. A research problem sets the overall direction and purpose of the study, while research questions focus on specific inquiries within the research problem. Both are crucial in guiding the research process, collecting relevant data, and generating new knowledge. By understanding the attributes of research problems and research questions, researchers can effectively design and conduct their studies, contributing to the advancement of knowledge in their respective fields.
Comparisons may contain inaccurate information about people, places, or facts. Please report any issues.
This paper is in the following e-collection/theme issue:
Published on 30.8.2024 in Vol 13 (2024)
EXploring Patterns of Use and Effects of Adult Day Programs to Improve Trajectories of Continuing Care (EXPEDITE): Protocol for a Retrospective Cohort Study
Authors of this article:
- Matthias Hoben 1, 2 , Dr rer medic ;
- Colleen J Maxwell 3, 4 , PhD ;
- Andrea Ubell 5, 6 , MSW ;
- Malcolm B Doupe 7, 8, 9 , PhD ;
- Zahra Goodarzi 10 , MD ;
- Saleema Allana 11 , PhD ;
- Ron Beleno 6 , BSc ;
- Whitney Berta 12 , PhD ;
- Jennifer Bethell 4, 12, 13 , PhD ;
- Tamara Daly 1, 6 , PhD ;
- Liane Ginsburg 1 , PhD ;
- Atiqur SM - Rahman 1 , PhD ;
- Hung Nguyen 1 , PhD ;
- Kaitlyn Tate 2 , PhD ;
- Kimberlyn McGrail 14 , PhD
1 School of Health Policy and Management, Faculty of Health, York University, Toronto, ON, Canada
2 Faculty of Nursing, College of Health Sciences, University of Alberta, Edmonton, AB, Canada
3 School of Pharmacy, University of Waterloo, Waterloo, ON, Canada
4 ICES, Toronto, ON, Canada
5 Alzheimer Society of York Region, Aurora, ON, Canada
6 Member of the Advisory Committee, Helen Carswell Chair in Dementia Care, Faculty of Health, York University, Toronto, ON, Canada
7 Max Rady Faculty of Health Sciences, College of Medicine, University of Manitoba, Winnipeg, MB, Canada
8 Manitoba Centre for Health Policy, Faculty of Health Sciences, University of Manitoba, Winnipeg, MB, Canada
9 Centre for Care Research, Western Norway University of Applied Sciences, Winnipeg, MB, Canada
10 Cumming School of Medicine, University of Calgary, Calgary, AB, Canada
11 Arthur Labatt Family School of Nursing, Faculty of Health Sciences, Western University, London, ON, Canada
12 Institute of Health Policy, Management and Evaluation, Dalla Lana School of Public Health, University of Toronto, Toronto, ON, Canada
13 KITE Research Institute, Toronto Rehabilitation Institute, University Health Network, Toronto, ON, Canada
14 Centre for Health Services and Policy Research, School of Population and Public Health, The University of British Columbia, BC, Canada
Corresponding Author:
Matthias Hoben, Dr rer medic
School of Health Policy and Management
Faculty of Health
York University
301E Strong College
4700 Keele Street
Toronto, ON, M3J 1P3
Phone: 1 437 335 1338
Email: [email protected]
Background: Adult day programs provide critical supports to older adults and their family or friend caregivers. High-quality care in the community for as long as possible and minimizing facility-based continuing care are key priorities of older adults, their caregivers, and health care systems. While most older adults in need of care live in the community, about 10% of newly admitted care home residents have relatively low care needs that could be met in the community with the right supports. However, research on the effects of day programs is inconsistent. The methodological quality of studies is poor, and we especially lack robust, longitudinal research.
Objective: Our research objectives are to (1) compare patterns of day program use (including nonuse) by province (Alberta, British Columbia, and Manitoba) and time; (2) compare characteristics of older adults by day program use pattern (including nonuse), province, and time; and (3) assess effects of day programs on attendees, compared with a propensity score–matched cohort of older nonattendees in the community.
Methods: In this population-based retrospective cohort study, we will use clinical and health administrative data of older adults (65+ years of age) who received publicly funded continuing care in the community in the Canadian provinces of Alberta, British Columbia, and Manitoba between January 1, 2012, and December 31, 2024. We will compare patterns of day program use between provinces and assess changes over time. We will then compare characteristics of older adults (eg, age, sex, physical or cognitive disability, area-based deprivation indices, and caregiver availability or distress) by pattern of day program use or nonuse, province, and time. Finally, we will create a propensity score–matched comparison group of older adults in the community, who have not attended a day program. Using time-to-event models and general estimating equations, we will assess whether day program attendees compared with nonattendees enter care homes later; use emergency, acute, or primary care less frequently; experience less cognitive and physical decline; and have better mental health.
Results: This will be a 3-year study (July 1, 2024, to June 30, 2027). We received ethics approvals from the relevant ethics boards. Starting on July 1, 2024, we will work with the 3 provincial health systems on data access and linkage, and we expect data analyses to start in early 2025.
Conclusions: This study will generate robust Canadian evidence on the question whether day programs have positive, negative, or no effects on various older adult and caregiver outcomes. This will be a prerequisite to improving the quality of care provided to older adults in day programs, ultimately improving the quality of life of older adults and their caregivers.
Trial Registration: ClinicalTrials.gov NCT06440447; https://clinicaltrials.gov/study/NCT06440447
International Registered Report Identifier (IRRID): PRR1-10.2196/60896
Introduction
Across the globe, societies are struggling to meet the needs of an aging population [ 1 - 5 ]. The increasing prevalence of dementia [ 6 - 8 ] and comorbid chronic conditions [ 9 , 10 ] lead to complex care needs [ 9 , 10 ] and to greater family or friend caregiver burden [ 11 - 14 ] (ie, “the extent to which caregivers perceive that caregiving has had an adverse effect on their emotional, social, financial, physical, and spiritual functioning” [ 15 ]). In response, health systems provide a range of ongoing care and supports to older adults and their caregivers—in Canada commonly referred to as continuing care [ 2 , 16 ]. Continuing care can be provided in an older adult’s private home, in the community (eg, an adult day program), or in a variety of congregate care settings including independent living, retirement homes, supportive or assisted living, or nursing homes (NHs) [ 17 , 18 ]. Governments have identified NHs as a major driver of public continuing care costs [ 17 , 19 - 21 ]. To mitigate pressures on public continuing care systems, and to meet aging in place preferences of older adults and their caregivers [ 22 - 24 ], reforms have implemented aging in place strategies. These strategies largely include (1) reserving NH care to those with the most complex care needs, and (2) improving access to an array of publicly funded continuing care options in the community [ 2 ].
Adult day programming is such a continuing care option to support aging in place [ 25 - 32 ]. Older adults in need of continuing care usually attend these programs for parts of the day, returning to their homes overnight (but overnight services are provided by some day programs). As this literature illustrates [ 25 - 32 ], the number of days a person attends a day program can vary widely, depending on the program and health jurisdiction, from a couple of days or month to daily attendance. The amount of time an individual attends also varies from a few hours or day to all day, or sometimes during nights, and so do admission criteria, supports and services offered, and funding models.
Despite these variations, day programs have unique characteristics that set them apart from other continuing care options. Day programs employ care staff and admit people with a certain level of support needs [ 30 , 33 ]. This distinguishes them from senior or community centers [ 34 ] and creative arts programs [ 35 ], which are open to independent older adults, do not employ care staff, and are organized more informally. Unlike home care [ 36 ] or in-home respite [ 37 ], day programs serve groups of older adults in a setting external to the attendee’s home [ 30 , 33 ], supporting social interactions and caregiver respite [ 32 ]. Unlike geriatric day hospitals, which provide medical, therapeutic, and rehabilitative care for a few weeks [ 38 ], day programs prioritize social and recreational activities, and they do so for long term (often for months or years) [ 30 , 33 ]. Day program services and supports usually include transportation; meals; recreational activities (eg, playing games, musical activities, crafting, and painting); socializing with other clients and day program staff; physical, cognitive, and spiritual activities; social work counseling; and case management support. Personal, nursing, and medical care are often not provided, or only to a limited extent, depending on the program and health system.
Recent literature reviews [ 28 - 32 , 39 ] reveal a growing body of evidence that suggests that day program attendance may be associated with attendees’ improved mental health, cognition, loneliness, quality of life, perceived health, physical functioning, use of polypharmacy, and mortality. These reviews also suggest that attendance may be associated with older adults’ delayed admissions to congregate care, reduced risk for hospitalization, improved caregiver burden, and caregivers’ feelings of competence, mental health, and well-being. However, reviews point to inconsistent findings, methodological limitations, and substantial heterogeneity of included studies. For example, a Canadian 1-group pre-post study suggested that Geriatric Depression Scale scores decreased (fewer depressive symptoms) from 5.0 at admission to a day program to 3.3 at discharge ( P =.007). A quasi-experimental study comparing depressive symptoms between day program attendees with dementia and nonattendees with dementia in the United States [ 40 ] found no group differences. However, on days of attendance, the proportion of caregivers who reported depressive symptoms for attendees decreased over time (from 32/133, 24% to 25/133, 19%; P <.02). A Canadian randomized controlled trial [ 41 ] found no difference in depressive symptoms between day program attendees and wait-listed nonattendees.
Across the literature, four key knowledge gaps persist: (1) we generally know little about the characteristics of day program attendees and nonattendees, or about those with different patterns of use. (2) We lack longitudinal data on changes in the aforementioned outcomes. (3) Generally, the methodological quality of available studies is poor [ 32 ], and we lack robust, large-scale, longitudinal evidence of older adult day programs on day program attendees—especially those living with dementia. With few notable exceptions [ 42 , 43 ], we especially lack current research on Canadian day programs with most research originating from the US or Canadian studies often dating back several decades [ 25 , 26 , 44 ]. (4) Differential effects of day programs on persons with multiple, intersecting vulnerabilities are poorly understood, despite inequity concerns [ 39 , 45 - 47 ]. Advanced age puts individuals at risk of ageism; physical and cognitive disabilities may expose them to ableism; the majority of older adults and their caregivers are women, often experiencing gender inequities; and giving and receiving care are associated with substantial health care costs, disproportionally affecting those with low income [ 48 ]. Racism or transphobia or homophobia can further increase these pressures, severely affecting older adults and their caregivers [ 49 , 50 ].
Our study will address these knowledge gaps comprehensively, rigorously, and simultaneously. We will address the following 3 research objectives:
- Explore patterns of day program use (eg, variations in time to first attendance, monthly hours of attendance, ongoing versus interrupted attendance, and total time of day program exposure), using latent class analyses (LCA), and compare the frequency of each latent use class between provinces and over time.
- Compare older adults’ demographic, social, and health characteristics (eg, age, sex, physical or cognitive disability, area-based deprivation indices, and caregiver availability or distress) by day program use or nonuse class, province, and time.
- Assess whether, compared with a propensity score–matched control group of nonattendees, day program attendees enter care homes at later points in time; use emergency, acute, or primary care less frequently; experience less cognitive and physical decline; have better mental health; and have less distressed caregivers. We will assess potential modification of these effects by day program use or nonuse class, age, sex, and social determinants of health (eg, area-based deprivation indices).
Study Design
Using an integrated knowledge translation (iKT) approach [ 51 , 52 ], we partnered with a cross-Canadian team of experts to design this population-based retrospective cohort study (ClinicalTrials.gov; NCT06440447) covering the Canadian provinces of Alberta, British Columbia, and Manitoba, and we will collaborate with our experts throughout the study. Experts include older adults (some with dementia), their caregivers, Alzheimer societies, caregiver organizations, day program staff and managers, and government and health system decision makers. They will provide intimate knowledge of day programs, and the experience of attending them or caring for an attendee, which will help us interpret and contextualize our findings. We will use deidentified clinical and health administrative data from each of the 3 provinces. Our study will follow the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) [ 53 ], and the REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) [ 54 ] guidelines. Provincial data policies require data to remain in each respective province, preventing linkage across provinces and analyses of all data in one place. Therefore, in-house data analysts with each provincial health system will carry out the analyses separately with shared protocols and programs.
Setting and Sample
Our study settings are community-based continuing care systems. Each province provides access to a range of publicly funded community-based continuing care services, including adult day programs [ 55 - 63 ]. Each provincial health system determines and enacts access criteria and provides services (directly or via contracted providers) [ 55 - 63 ]. Day program eligibility is assessed in each province, using comparable processes, criteria, and assessments (ie, the Resident Assessment Instrument—Home Care [RAI-HC], a standardized, valid, reliable assessment tool [ 64 ]) [ 60 , 65 , 66 ]. To be eligible, attendees need to have not only some care dependency but also the ability to cope to some extent with activities of daily living, ambulate or transfer with no or minimal assistance, be continent or independent in managing continence products, exhibit no or easily manageable responsive behaviors, and either be alone for extended periods or have a caregiver who requires respite. Our study cohort will include all individuals aged 65 years or older with an initial RAI-HC assessment completed between January 1, 2012, and December 31, 2021. We will follow everyone until they move into a care home, are lost to follow-up (eg, because of death, moving out of province, loss of public insurance eligibility), or until December 31, 2024 (the end of the period covered by our data). That will allow for a care trajectory of at least 3 years (for those with an initial RAI-HC assessment in December 2021), enabling us to assess the number and characteristics of individuals with different day program use patterns, and compare them with those who were never exposed to a day program.
Sample Size Calculation
The yearly average number of completed RAI-HC assessments is ~20,000-30,000 in Alberta, ~34,000-39,000 in British Columbia, and ~10,000 in Manitoba [ 67 ]. About 50% of those assessed receive a reassessment within 12 months and another 10%-30% receive a reassessment after >15 months [ 68 ]. There are 89 publicly subsidized day programs in Alberta (~3300 spaces per day), 95 in British Columbia (~1500 spaces per day), and 70 in Manitoba (~1000 spaces per day) for a total of 254-day programs with 5800 spaces on any given day. Some day program users do not attend daily, but only 1 or a few days per week, so the number of unique attendees exceeds the number of spaces per day. This corresponds to >20,000 attendees per year (>200,000 within the study period), each with multiple assessments. Our study sample size will be large enough to detect small effects sizes. With Cox proportional hazards models, adjusted for covariates explaining an assumed 25% of effect variance (a=.05; power=0.8) [ 69 ], we require a total sample of 1327 participants to detect a hazard ratio for admissions to care homes of 0.6 (as can be expected based on a similar Canadian study [ 42 ]) in favor of day program attendees. Similarly, Kelly [ 43 ] was able to detect significantly fewer emergency department visits and hospital admissions per day among 812 day program attendees compared with 812 propensity score matched to nonattendees. Our expected sample size will be considerably larger than for those previous studies, allowing for complex statistical modeling.
Data Sources
For each individual in our cohort, designated provincial health system analysts will link all records available within the study time frame from the following databases: (1) regional continuing care registries, documenting when an individual starts or stops receiving any community-based continuing care, including day programs, how these services change over time, and when an individual is admitted to a care home. (2) Population registries for each participant’s demographic data. (3) RAI-HC assessments [ 64 ], completed annually for people receiving long-term home care (60+ days), and to determine day program eligibility. The RAI-HC will provide data on older adults’ medical conditions, functional dependence, pain, cognitive impairment, mood, and behavioral problems. It also includes information on a person’s marital or partnership status, caregiver availability, whether that caregiver lives with the older adult, and caregiver distress. Additional caregiver characteristics are not included in the available provincial databases, posing a limitation to our quantitative analyses. However, a related prospective cohort study that we are conducting in Ontario will allow us to link comprehensive caregiver and older adult data, and we are currently conducting additional qualitative research that will illuminate how caregiver characteristics may affect day program use and outcomes. (4) Discharge abstract database (DAD) for information on all inpatient hospital stays, including diagnoses and length of stay. (5) National Ambulatory Care Report System (NACRS) for all emergency department visits and diagnoses. In British Columbia, we will use the physician payment file in addition, since NACRS is not collected in all emergency departments [ 70 ]. (6) Pharmaceutical information on outpatient prescription medications filled through a community pharmacy and covered by provincial drug formulary. (7) Care provider claims data for health service claims submitted for payment by health care providers (eg, general practitioners, nurse practitioners, geriatricians, geriatric psychiatrists, neurologists, therapists) to obtain information on general and specialist health services used by participants.
Study Variables
Our exposure will be different patterns of day program use or nonuse, based on information from the provincial continuing care registries, documenting the dates a person starts or stops attending a day program, days of attendance, and the duration of each visit. Day program use patterns will be determined, using LCAs (see Statistical Analyses section) [ 71 ]. We will categorize three continuous variables as low, low-moderate, high-moderate, or high use, using sample distribution quartiles: (1) time between first RAI-HC assessment and first attendance of a day program; (2) average number of hours of day program attendance (ie, total number of hours spent in a day program divided by the number of times attended); and (3) total number of days a person attended a day program. LCAs will also include a categorical variable, indicating whether a person consistently attended a day program or whether there were longer periods (several weeks) of nonattendance. Nonuse will be defined as no day program exposure at any time during a person’s continuing care trajectory.
Study Outcomes
The data sources noted above enable us to examine a range of important study outcomes. Data on the time between a person’s first RAI-HC assessment and admission to a care home will come from provincial continuing care registries. Symptoms of depression will be assessed using the validated RAI-HC Depression Rating Scale [ 72 ], with scores ranging from 0 to 14 and a cut point of 3 or higher representing clinically meaningful depressive symptoms [ 72 , 73 ]. We will capture physical and cognitive decline, using validated RAI-HC scales [ 64 ]: the Activities of Daily Living Hierarchy (ADLh) Scale [ 74 ] and the Cognitive Performance Scale (CPS) [ 75 ]. Both scales range from 0 (no impairment) to 6 (maximum impairment), and our outcomes will be dichotomous, indicating any increase (vs no change or a decrease) between the previous and follow-up measurement in each of these scales. Using care practitioner claims data, we will generate rates of different types of primary and specialist care use (eg, family physician, specialists, nursing practitioner, and allied health providers). We will use the DAD and NACRS databases to generate rates of emergency department registrations, hospital admissions, and days in hospital (including alternative level of care) [ 43 ]. Rates will be stratified by day program use or nonuse pattern.
Demographic, Social, and Health Characteristics
These will include older adults’ age, sex, marital or partnership status (population registries and RAI-HC), physical disability (ADLh Scale score of >3), and cognitive impairment (CPS score of >3). Available data sets include only a binary variable on biological sex (male or female) and no nonbinary information on gender identity. We will also include RAI-HC measures of caregiver availability (item G1e) and burden (items G2a-c). Finally, we will include 4 publicly available area-level measures from the Canadian Index of Multiple Deprivation [ 76 , 77 ]: residential instability (eg, housing insecurity, overcrowding, and frequent moves), economic dependency (high number of older adults, children younger than 15 years, and persons receiving government transfers), ethnocultural composition (eg, immigrants and racialized individuals), and situational vulnerability (eg, indigenous peoples, dwellings needing major repairs, and low education). Using Statistics Canada data, each measure is derived for 54,775 geographical dissemination areas, using 17 variables. Quintile-based ranks for each of the indices (1=least deprived to 5=most deprived) will be assigned to individuals based on their home’s postal code [ 77 ].
Propensity Score–Matching Variables
To compare outcomes between day program attendees and nonattendees, we will use propensity score matching [ 78 ] (for details, see Statistical Analyses section). Propensity scores aim to ensure a similar distribution of baseline variables among treatment (day program attendees) and control (nonattendees)—akin to what random assignment aims to accomplish in randomized trials [ 78 ]. Since we lack evidence on differences between day program attendees and nonattendees, our objective 2 analyses will be key to informing the selection of the exact covariates that will form the propensity score. We will derive covariates for day program attendees from the RAI-HC day program eligibility assessment (index date). For each day program attendee, we will identify potential matches as nonattendees whose first RAI-HC assessment was completed within ±3 months of the attendee’s index date (ie, admission to long-term home care at about the same time). This RAI-HC assessment will provide the relevant covariates to enable propensity score matching with day program attendees as of their index date.
Our first set of matching covariates will be RAI-HC variables used by health systems to determine day program eligibility [ 60 , 65 , 66 ]: physical functioning (ADLh Scale), cognition (CPS), behavioral symptoms (Aggressive Behavior Scale [ 79 ]), bladder or bowel continence (items I1, I3), availability of a caregiver (item G1e), and caregiver distress (items G2a-c). This will ensure that control participants are potentially eligible to a day program. Possible reasons for nonattendance include the lack of day program spaces, preference not to attend, inability to afford the required copayments, or not receiving a day program referral. Our experts assure us that the pool of potential matches far exceeds that of attendees, supporting the feasibility of this study and underscoring the lack of day program spaces. This approach excludes individuals whose care needs are either too low or too severe for day program eligibility, but it minimizes confounding by the matched variables and ensures comparable groups at baseline [ 80 - 82 ]. Finally, we will include a second set of matching covariates: health and social characteristics identified in objective 2 by which attendees and potentially eligible nonattendees differ and that overlap sufficiently between attendees and nonattendees (eg, age, sex, type or duration of publicly funded community care received before the matching index date, and deprivation indices).
Additional Covariates
Additional covariates for model adjustment will come from RAI-HC, DAD, NACRS, pharmaceutical, and claims records (eg, geriatric syndromes, medical diagnoses, and prescribed medications). We might also adjust for additional community care services (eg, in-home respite and home care).
Statistical Analyses
Objective 1: explore patterns of day program use.
Using our day program cohort, we will conduct LCAs to determine the number of different day program use patterns, using the 4 variables described in the exposures section. LCAs are widely used to identify subgroups by clusters of characteristics (ie, parameters of day program use) [ 71 ]. In collaboration with our experts and guided by relevant literature, we will prespecify the expected number of classes. We will carry out LCAs separately in each province. We will run models with the prespecified number of classes, and with 1, 2, and 3 more and fewer classes than the number prespecified [ 71 ]. We will compare the fit between models, using bootstrap likelihood ratio tests [ 71 ], and select a final model that reflects the same number and types of classes in each province, balancing theoretical, conceptual, and statistical considerations. To assess temporal changes in the number of day program attendees within each use pattern, and differences between provinces, we will report and graphically plot the proportion (95% CI) of individuals within each latent class by quarter and province.
Objective 2: Compare Older Adults’ Characteristics by Day Program Use, Province, and Time
Using our full cohort of day program attendees and nonattendees, we will descriptively assess the distribution of sample characteristics over time and by province. In each province and quarter, we will report and plot graphically the proportion (95% CI) of individuals with each characteristic, stratified by day program use class versus nonuse. Using general estimating equations (GEEs) [ 83 ], we will assess whether the number of persons with each characteristic has changed over time and whether characteristics are associated with older adults’ day program use or nonuse pattern. We will run a separate GEE model for each characteristic within each province, with the respective characteristic as individual-level outcome. We will run binary logistic regressions for dichotomous variables (eg, sex) and ordinal regressions for categorical variables (eg, residential instability quintile). Models will account for repeated measures within individuals and include the independent variables year of assessment (to assess change in social determinants over time), use or nonuse class (to assess differences in social determinants by day program use), and an interaction between year and use or nonuse (to assess how social determinants differed between use and nonuse patterns by year). Using random-effects mixed regression models, we will pool provincial effects statistically. Other Pan-Canadian studies, such as the Canadian Network for Observational Drug Effect Studies [ 84 ], have successfully applied this approach and developed rigorous protocols to minimize bias and maximize consistency of regional analyses.
Objective 3: Assess Effects of Day Programs
To create a propensity score, we will run a logistic regression for each province with day program attendance or nonattendance as the dependent variable and adding matching covariates. We will use one-to-one matching (1 matched nonattendee for every attendee) [ 78 ]. We will use matching without replacement [ 85 ] and apply an optimal caliper matching algorithm [ 86 ]. As per best practice recommendations [ 87 ], we will use a caliper width of 0.2 of the SD of the propensity score’s logit. If this matching approach does not allow us to achieve a sufficient sample size, we will use propensity score quintiles for matching.
We will compare sample characteristics and study outcomes between attendees and nonattendees in every year and province, using bivariate statistical tests (eg, chi-square test or Fisher exact test for categorical variables, t tests, or ANOVAs for continuous variables, and their nonparametric equivalents if variables violate statistical assumptions). To assess the effect of day program exposure on time to care home admission, we will specify a multilevel time-to-event model with a health region–level random effect [ 88 ]. Health systems in each of the 3 provinces are divided into 5 health regions [ 89 - 91 ], and regional policies may cause clustering effects that our models must account for. Each model will include day program use or nonuse class as independent variable and will be adjusted for time-varying variables. These will include matching variables, if appropriate (ie, in case of group differences in matching variables over time or due to missing data) [ 80 - 82 ] and, if needed, additional covariates (eg, demographics, social determinants, medical or functional conditions, and non–day program community care). Covariates that differ between attendees and nonattendees with a P value of ≤.15 in the bivariate analyses will be considered for inclusion. We will add covariates stepwise, one-by-one, and remove those that cause collinearity issues or decrease model fit. As in objective 2, we will pool provincial effects statistically, using random-effects mixed regression models.
Using GEEs and a similar approach as for the time-to-event models (including separate models in each province and statistical pooling of their effects), we will assess whether the other study outcomes differ by day program use or nonuse pattern. Models will include each study outcome of interest as a dependent variable, day program use or nonuse class and time of assessment as independent variables, and similar covariates (using the same stepwise approach) as the time-to-event models. Models will also include a random term to account for repeated measures within individuals. The choice of a link function will be informed by the nature of the variable and theoretical and empirical considerations. For example, the number of hospital, emergency department, or physician visits has been shown to follow a zero-inflated negative binomial distribution, sometimes requiring an offset for the natural logarithm of person-time [ 92 ]. For continuous outcomes (eg, days spent in hospitals), we will use an identity link function, and for dichotomous outcomes (eg, presence or absence of depressive symptoms), we will use a logit link function. All models will apply multiple imputation in case of missing data, which we expect to be small based on our previous work with the administrative health care data sources used in this study.
Ethical Considerations
We received ethics approvals from the York University Ethics Review Board, Human Participants Review Sub-Committee (e2022-412, December 1, 2022), the University of Alberta Health Research Ethics Board—Health Panel (Pro00127850, February 3, 2023), and the University of British Columbia Research Ethics Board (H24-01435, August 1, 2024), and we are in the process of obtaining ethics approval from the University of Manitoba Health Research Ethics Board.
Funded by an endowed research chair, the Helen Carswell Chair in Dementia Care (July 1, 2022, to June 30, 2027), this will be a 3-year study (July 1, 2024, to June 30, 2027). Starting on July 1, 2024, we will work with the 3 provincial health systems on data access and linkage, and we expect data analyses to start in early 2025.
Principal Findings
Older adults, caregivers, and health systems urgently need solutions to empower older adults to receive care at home for longer [ 93 ]. There are few feasible solutions that target both, the older adult in need of care and their family or friend caregiver, but day programs are one of them [ 30 , 33 ]. Despite the knowledge that day programs could fill an immense and costly care gap [ 27 - 33 , 37 , 39 , 45 - 47 , 94 , 95 ], we lack the research needed to inform policy and drive practice change to make day programs more available [ 30 , 33 ]. This study will generate robust Canadian knowledge on whether day programs have positive, negative, or no effects on outcomes that matter most to older adults, their caregivers, and health systems. For example, day programs aim to support older adults and their caregivers to avoid or delay care home admissions; reduce or avoid costly and unnecessary emergency, acute, or primary care use; and improve the health and well-being of older adults and their caregivers [ 27 - 33 , 37 , 39 , 45 - 47 , 94 , 95 ]. However, the international research is inconclusive on whether or not day programs are effective in accomplishing these aims [ 27 - 33 , 37 , 39 , 45 - 47 , 94 , 95 ], and we especially lack robust, longitudinal, and cross-provincial Canadian research [ 25 , 26 , 44 ]. Therefore, this study will provide critical knowledge that is urgently needed by health systems. First, we will determine how many persons are attending day programs in the 3 participating Canadian provinces, what their patterns of use look like, whether these patterns have changed over time, and similarities and differences of these patterns between provinces. Second, we will assess how characteristics of older adults who attend day programs differ from those who do not attend day programs. Finally, we will assess whether day programs are effective in delaying admissions to care homes, reducing emergency, acute and primary care, and in improving various outcomes related to older adults’ health and well-being.
Our iKT approach, in which we have been closely partnering with older adults (some with dementia), their caregivers, Alzheimer societies, caregiver organizations, day program staff and managers, and government and health system decision makers, will ensure that our research addresses issues that these groups have deemed a priority. It will further facilitate rapid translation of these findings into policy and practice changes. Results will be disseminated in a variety of ways. Staying true to our iKT approach, we will invite, encourage, and empower our experts to participate in, coauthor, or lead these activities (to the extent our experts wish to be involved and have capacity to do so).
Limitations
While this study has various important strengths, including the use of comprehensive, population-based, cross-provincial health administrative data, and application of robust statistical methods, there are some limitations. First, important variables, such as older adult quality of life, various social determinants of health, or day program characteristics, are not available in the administrative health care data available to us. Second, the health administrative data used in this study do not allow for identification of caregiver health administrative data, preventing linkage of caregiver and older adult data. Therefore, our team currently also carries out a prospective cohort study (ClinicalTrials.gov; NCT06496945) in which we will collect these missing variables to fill the mentioned gaps. Finally, quantitative data may suggest the presence or absence of an effect, but they may be more limited in explaining the mechanisms leading up to the effect or the reasons of the lack of an effect. Our program of research includes a realist literature review and comprehensive qualitative work to address the lived experience of older adults and their caregivers in day programs and the “how and why” of day program effects (or the lack thereof).
In webinars in years 2 and 3, researchers, trainees, and experts will copresent key research findings on specific topics, such as effects of day programs in general (ie, on individuals with dementia, caregivers, and health systems); variation of day program effects in various equity-deserving groups or by day program characteristics; or jurisdictional differences in day program structures, policies, characteristics, and effects. Thirty to 50 additional experts (not members of our advisory committee) will be invited to participate per webinar, including provincial or regional health system policy makers, Alzheimer Societies, caregiver organizations, day program operators or managers or staff, individuals with dementia, and caregivers. In particular, webinars will offer the opportunity for discussion about relevance of findings within and across jurisdictions and for cross-provincial learning (learning health systems).
Researcher, trainee, and expert team members will also codevelop a series of briefing documents that highlight key messages of our research. Documents will target health system policy makers and day program operators and managers. They will be a valuable tool to support desired directions and action post project funding. In year 2, we will hold a series of workshops to engage experts in a facilitated, deliberative process of developing alternative approaches that improve day program effects on individuals with dementia, their caregivers, and health systems.
We are planning the preparation of several peer-reviewed manuscripts (cocreated by researchers, trainees, and experts). Publications might include (among others) (1) this research protocol of our study; (2) a manuscript comparing the number and characteristics of day program attendees over time and across participating regions; (3) a comparison of older adults by day program use or nonuse stratified by health region; and (4) several papers (~3-5) on the effects of day programs on older adults. Team members will give presentations at conferences within Canada (eg, Canadian Association for Health Services and Policy Research, Ontario Long Term Care Association, National Health Leadership Conference, Canadian Alliance for Long Term Care, Canadian Association on Gerontology, and Congress of the Humanities and Social Sciences) and internationally (Gerontological Society of America, International Association of Gerontology and Geriatrics). Experts will be invited to participate in symposia, copresent, or lead presentations.
In year 3, key messages will be used to develop various lay summaries and an easily accessible, animated summary project video that can also be used for educational training on aging in place and care of individuals with dementia and their caregivers in the community. These will be posted on our study website and on our team members websites.
In conclusion, this study will identify essential elements of day programs and how they can be improved. We will provide critical evidence for health systems to help them leverage the full potential of day programs to provide appropriate care, prevent inequities, and mitigate the need for emergency, hospital, and congregate care. Ultimately, we will improve the quality of life of older adults (including those with dementia) and their caregivers, alleviate caregiver burden, and reduce social costs associated with poor health and well-being. Future studies will expand this research to additional health jurisdictions.
Acknowledgments
We would like to thank all members of the Helen Carswell Chair in Dementia Care Advisory Committee, who helped us identify important research priorities (including the population-based, retrospective cohort study proposed here) and in conceptualizing and designing this study. This study is funded by the Carswell Family Foundation, which funds the Helen Carswell Chair in Dementia Care, held by MH. The funder has had no role in designing this study and preparing or approving this publication, and the funder will have no role in accessing and analyzing the administrative health care data, and in publishing or approving future manuscripts.
Data Availability
This study uses population-based clinical and administrative health care data, routinely collected, and owned by the participating health regions. Provincial data policies do not allow for public sharing or access of these data. Data are not allowed to be removed from regional repositories. Guided by the study team, data in each region will be analyzed by health data analysts employed by the respective health care system. Study findings will then be pooled across health regions, using shared protocols and statistical codes. Access may be granted to those who meet prespecified criteria for access, available at on the websites of (1) the Alberta SPOR SUPPORT Unit (AbSPORU) [ 96 ] (email: [email protected]), (2) Population Data BC [ 97 ] (email: [email protected]), and (3) Shared Health Inc [ 98 ] (email: [email protected]).
Authors' Contributions
MH is the lead investigator of this study, and CJM, AU, MBD, ZG, and SA are coleads. MH, CJM, AU, MBD, ZG, SA, RB, WB, JB, TD, LG, HN, ASMR, KT, and KG helped conceptualize the study and to design the study methods. MH wrote the original draft, and CJM, AU, MBD, ZG, SA, RB, WB, JB, TD, LG, HN, ASMR, KT, and KG critically reviewed and edited various iterations of the manuscript. All authors approve of the manuscript in its current form and agree to be accountable for all of its contents.
Conflicts of Interest
None declared.
- European Commission. The 2018 Ageing Report: Economic and Budgetary Projections for the 28 EU Member States (2016-2070). Luxembourg. European Commission; 2018.
- Federal/Provincial/Territorial Ministers Responsible for Seniors. Core Community Supports to Age in Community. Ottawa. Government of Canada; 2019.
- MacDonald BJ, Wolfson M, Hirdes JP. The Future Co$t of Long-Term Care in Canada. Toronto, ON. National Institute on Aging; 2019.
- Thomas KS, Applebaum R. Long-term services and supports (LTSS): a growing challenge for an aging America. Public Policy Aging Report. 2015;25(2):56-62. [ CrossRef ]
- Whitman DB. Unsolved mysteries in aging policy. Public Policy Aging Report. 2015;25(2):67-73. [ CrossRef ]
- Alzheimer's Association. 2022 Alzheimer's disease facts and figures. Alzheimer Dement. 2022;18(4):700-789. [ CrossRef ]
- Prince MJ, Wimo A, Guerchet MM, Ali GC, Wu YT, Prina M. World Alzheimer Report 2015—The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends. London. Alzheimer's Disease International; 2015.
- Government of Canada. Dementia in Canada. Ottawa. Public Health Agency of Canada URL: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/dementia.html [accessed 2022-09-02]
- Nguyen H, Manolova G, Daskalopoulou C, Vitoratou S, Prince M, Prina AM. Prevalence of multimorbidity in community settings: a systematic review and meta-analysis of observational studies. J Comorb. 2019;9:2235042X19870934. [ FREE Full text ] [ CrossRef ] [ Medline ]
- The Academy of Medical Sciences. Multiple Long-Term Conditions (Multimorbidity): A Priority for Global Health Research. London. The Academy of Medical Sciences; 2018. URL: https://acmedsci.ac.uk/policy/policy-projects/multimorbidity [accessed 2022-09-02]
- Canadian Institute for Health Information (CIHI). Quick stats—home care reporting system (HCRS) profile of clients in home care 2020-2021. CIHI. URL: https://www.cihi.ca/en/quick-stats [accessed 2022-09-02]
- Morgan T, Ann Williams L, Trussardi G, Gott M. Gender and family caregiving at the end-of-life in the context of old age: a systematic review. Palliat Med. 2016;30(7):616-624. [ CrossRef ] [ Medline ]
- Quesnel-Vallée A, Willson A, Reiter-Campeau S. Health inequalities among older adults in developed countries: reconciling theories and policy approaches. In: George L, Ferraro K, editors. Handbook of Aging Social Sciences. London. Elsevier; 2016:483-502.
- Quesnel-Vallée A, Farrah J, Jenkins T. Population aging, health systems, and equity: Shared challenges for the United States and Canada. In: Settersten Jr RA, Angel JL, editors. Handbook of Sociology of Aging. New York, Dordrecht, Heidelberg, London. Springer; 2011:563-581.
- Zarit SH, Todd PA, Zarit JM. Subjective burden of husbands and wives as caregivers: a longitudinal study. Gerontologist. 1986;26(3):260-266. [ CrossRef ] [ Medline ]
- McGrail K. Long-term care as part of the continuum. Healthc Pap. 2011;10(4):39-43; discussion 58-62. [ CrossRef ] [ Medline ]
- Sinha S, Dunning J, Wong I, Nicin M, Nauth S. Enabling the Future Provision of Long-term Care in Canada. Toronto, ON. National Institute on Aging; 2019.
- Government of Canada. Federal/provincial/territorial ministers responsible for seniors. Report on housing needs of seniors. Ottawa. Government of Canada; 2019. URL: https://www.canada.ca/en/employment-social-development/corporate/seniors/forum/report-seniors-housing-needs.html [accessed 2022-09-02]
- Spasova S, Baeten R, Coster S, Ghailani D, Peña-Casas R, Vanhercke Art. Challenges in Long-Term Care in Europe—A Study of National Policies 2018. Brussels. European Commission; 2018. URL: https://ec.europa.eu/social/main.jsp?langId=en&catId=1135&newsId=9185&furtherNews=yes [accessed 2022-09-02]
- Gonçalves J, Weaver F, Konetzka RT. Measuring state medicaid home care participation and intensity using latent variables. J Appl Gerontol. 2020;39(7):731-744. [ CrossRef ] [ Medline ]
- Wysocki A, Butler M, Kane RL, Kane RA, Shippee T, Sainfort F. Long-term services and supports for older adults: a review of home and community-based services versus institutional care. J Aging Soc Policy. 2015;27(3):255-279. [ CrossRef ] [ Medline ]
- Royal Bank of Canada. 2013 RBC retirement myths & realities poll: most appealing living arrangements for boomers. 2013. URL: http://www.rbc.com/newsroom/news/2013/20131024-myths-realities.html [accessed 2022-09-02]
- American Association of Retired Persons (AARP). 2018 home and community preferences: a national survey of adults age 18-plus. Washington, DC. AARP Research; 2018. URL: https://www.aarp.org/research/topics/community/info-2018/2018-home-community-preference.html [accessed 2022-09-02]
- European Commission. Health and long-term care in the European Union. Luxembourg. European Commission; 2007. URL: https://sid-inico.usal.es/idocs/F8/FDO22761/health_european_union.pdf [accessed 2022-09-02]
- Gutman GM, Milstein S, Killam J, Lewis D, Hollander MJ. Adult day care centres in British Columbia: models, characteristics and services. Health Rep. 1993;5(2):189-207. [ Medline ]
- Gutman GM, Milstein S, Killam J, Lewis D, Hollander MJ. Adult day care centres in British Columbia: client characteristics, reasons for referral and reasons for non-attendance. Health Rep. 1993;5(3):321-333. [ Medline ]
- Mason A, Weatherly H, Spilsbury K, Arksey H, Golder S, Adamson J, et al. A systematic review of the effectiveness and cost-effectiveness of different models of community-based respite care for frail older people and their carers. Health Technol Assess. 2007;11(15):1-157, iii. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Fields NL, Anderson KA, Dabelko-Schoeny H. The effectiveness of adult day services for older adults: a review of the literature from 2000 to 2011. J Appl Gerontol. 2014;33(2):130-163. [ CrossRef ] [ Medline ]
- Tretteteig S, Vatne S, Rokstad AMM. The influence of day care centres for people with dementia on family caregivers: an integrative review of the literature. Aging Ment Health. 2016;20(5):450-462. [ CrossRef ] [ Medline ]
- Ellen ME, Demaio P, Lange A, Wilson MG. Adult day center programs and their associated outcomes on clients, caregivers, and the health system: a scoping review. Gerontologist. 2017;57(6):e85-e94. [ CrossRef ] [ Medline ]
- Orellana K, Manthorpe J, Tinker A. Day centres for older people: a systematically conducted scoping review of literature about their benefits, purposes and how they are perceived. Ageing Soc. 2020;40(1):73-104. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Lunt C, Dowrick C, Lloyd-Williams M. What is the impact of day care on older people with long-term conditions: a systematic review. Health Soc Care Community. 2021;29(5):1201-1221. [ CrossRef ] [ Medline ]
- Symonds-Brown H, Ceci C, Duggleby W, Purkis ME. Re-thinking the nature of day programs for people with dementia: implications for research. Dementia (London). 2021;20(1):326-347. [ CrossRef ] [ Medline ]
- Song M, Seo K, Choi S, Choi J, Ko H, Lee SJ. Seniors centre-based health intervention programmes in the United States and South Korea: a systematic review. Int J Nurs Pract. 2017;23(5). [ CrossRef ] [ Medline ]
- Bellazzecca E, Teasdale S, Biosca O, Skelton DA. The health impacts of place-based creative programmes on older adults' health: a critical realist review. Health Place. 2022;76:102839. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Johnson S, Bacsu J, Abeykoon H, McIntosh T, Jeffery B, Novik N. No place like home: a systematic review of home care for older adults in Canada. Can J Aging. 2018;37(4):400-419. [ CrossRef ] [ Medline ]
- Vandepitte S, Van Den Noortgate N, Putman K, Verhaeghe S, Faes K, Annemans L. Effectiveness of supporting informal caregivers of people with dementia: a systematic review of randomized and non-randomized controlled trials. J Alzheimers Dis. 2016;52(3):929-965. [ CrossRef ] [ Medline ]
- Hoe J, Ashaye K, Orrell M. Don't seize the day hospital! Recent research on the effectiveness of day hospitals for older people with mental health problems. Int J Geriatr Psychiatry. 2005;20(7):694-698. [ CrossRef ] [ Medline ]
- Manthorpe J, Moriarty J. Examining day centre provision for older people in the UK using the equality act 2010: findings of a scoping review. Health Soc Care Community. 2014;22(4):352-360. [ CrossRef ] [ Medline ]
- Femia EE, Zarit SH, Stephens MAP, Greene R. Impact of adult day services on behavioral and psychological symptoms of dementia. Gerontologist. 2007;47(6):775-788. [ CrossRef ] [ Medline ]
- Baumgarten M, Lebel P, Laprise H, Leclerc C, Quinn C. Adult day care for the frail elderly: outcomes, satisfaction, and cost. J Aging Health. 2002;14(2):237-259. [ CrossRef ] [ Medline ]
- Kelly R, Puurveen G, Gill R. The effect of adult day services on delay to institutional placement. J Appl Gerontol. 2016;35(8):814-835. [ CrossRef ] [ Medline ]
- Kelly R. The effect of adult day program attendance on emergency room registrations, hospital admissions, and days in hospital: a propensity-matching study. Gerontologist. 2017;57(3):552-562. [ CrossRef ] [ Medline ]
- Molzahn AE, Gallagher E, McNulty V. Quality of life associated with adult day centers. J Gerontol Nurs. 2009;35(8):37-46. [ CrossRef ] [ Medline ]
- Manthorpe J, Moriarty J. Opportunity knocks: exploring the links between day opportunities and equal opportunities. Practice. 2013;25(5):317-333. [ CrossRef ]
- Sadarangani TR, Murali KP. Service use, participation, experiences, and outcomes among older adult immigrants in American adult day service centers: an integrative review of the literature. Res Gerontol Nurs. 2018;11(6):317-328. [ CrossRef ] [ Medline ]
- Li Y, Liu J, Sun F, Xu L. Adult day service use among minority older adults: facilitators, barriers, and outcomes from an updated integrative literature review between 2010 to 2021. J Appl Gerontol. 2022;41(10):2253-2263. [ CrossRef ] [ Medline ]
- Rushford N, Harvey D. Dementia as a disability and human rights issue. Healthc Pap. 2016;16(2):45-51. [ FREE Full text ] [ CrossRef ]
- Forrester SN, Gallo JJ, Whitfield KE, Thorpe RJ. A framework of minority stress: from physiological manifestations to cognitive outcomes. Gerontologist. 2019;59(6):1017-1023. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Fredriksen-Goldsen KI, Kim HJ. The science of conducting research with LGBT older adults—an introduction to aging with pride: national health, aging, and sexuality/gender study (NHAS). Gerontologist. 2017;57(suppl 1):S1-S14. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Leggat FJ, Wadey R, Day MC, Winter S, Sanders P. Bridging the know-do gap using integrated knowledge translation and qualitative inquiry: a narrative review. Qual Res Sport Exerc Health. 2021;15(2):188-201. [ CrossRef ]
- Boyko JA, Riley BL, Willis CD, Stockton L, Zummach D, Kerner J, et al. Knowledge translation for realist reviews: a participatory approach for a review on scaling up complex interventions. Health Res Policy Syst. 2018;16(1):101. [ FREE Full text ] [ CrossRef ] [ Medline ]
- von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. STROBE Initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453-1457. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Benchimol EI, Smeeth L, Guttmann A, Harron K, Moher D, Petersen I, et al. RECORD Working Committee. The reporting of studies conducted using observational routinely-collected health data (RECORD) statement. PLoS Med. 2015;12(10):e1001885. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Home care services in Manitoba. Province of Manitoba—Health. Government of Manitoba. URL: https://www.gov.mb.ca/health/homecare/index.html [accessed 2023-06-28]
- Home care. Winnipeg Regional Health Authority. URL: https://wrha.mb.ca/home-care/ [accessed 2023-06-28]
- Alberta regulation 296/2003, public health act, co-ordinated home care program regulation. Government of Alberta. 2022. URL: https://kings-printer.alberta.ca/570.cfm?frm_isbn=9780779830787&search_by=link [accessed 2023-06-28]
- Continuing care—overview. Government of Alberta. URL: https://www.alberta.ca/about-continuing-care.aspx [accessed 2023-06-28]
- Alberta Health Services. Home & community care. URL: https://www.albertahealthservices.ca/cc/Page15488.aspx [accessed 2023-06-28]
- Adult day programs. Alberta Health Services. URL: https://www.albertahealthservices.ca/cc/Page15504.aspx [accessed 2023-06-28]
- Continuing Care Act. Government of British Columbia. URL: https://www.bclaws.gov.bc.ca/civix/document/id/complete/statreg/96070_01 [accessed 2023-06-28]
- British Columbia Ministry of Health. Home & Community Care—Province of British Columbia. URL: https://www2.gov.bc.ca/gov/content/health/accessing-health-care/home-community-care [accessed 2023-06-28]
- Adult day services—Province of British Columbia. British Columbia Ministry of Health. URL: https://www2.gov.bc.ca/gov/content/health/accessing-health-care/home-community-care/care-options-and-cost/adult-day-services [accessed 2023-06-28]
- Hogeveen SE, Chen J, Hirdes JP. Evaluation of data quality of interRAI assessments in home and community care. BMC Med Inform Decis Mak. 2017;17(1):150. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Adult day services—Province of British Columbia. Ministry of Health, British Columbia. URL: https://www2.gov.bc.ca/gov/content/health/accessing-health-care/home-community-care/care-options-and-cost/adult-day-services [accessed 2023-11-28]
- Winnipeg Regional Health Authority. Home Care Case Coordinator Procedures Manual. Winnipeg, MB. Winnipeg Regional Health Authority; 2016.
- Canadian Institute for Health Information (CIHI). Quick stats | CIHI | home care reporting system. URL: https://www.cihi.ca/en/quick-stats [accessed 2023-04-27]
- Canadian Institute for Health Information (CIHI). Home Care Reporting System Data Users Guide 2020-2021. Ottawa, ON. Canadian Institute for Health Information (CIHI); 2022.
- Hsieh FY, Lavori PW. Sample-size calculations for the cox proportional hazards regression model with nonbinary covariates. Control Clin Trials. 2000;21(6):552-560. [ CrossRef ] [ Medline ]
- Peterson S, Wickham M, Lavergne R, Beaumier J, Ahuja M, Mooney D, et al. Methods to Comprehensively Identify Emergency Department Visits Using Administrative Data in British Columbia. Vancouver, BC. Centre for Health Services and Policy Research, School of Population and Public Health, University of British Columbia; 2021.
- Dziak JJ, Lanza ST, Tan X. Effect size, statistical power and sample size requirements for the bootstrap likelihood ratio test in latent class analysis. Struct Equ Modeling. 2014;21(4):534-552. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Burrows AB, Morris JN, Simon SE, Hirdes JP, Phillips C. Development of a minimum data set-based depression rating scale for use in nursing homes. Age Ageing. 2000;29(2):165-172. [ CrossRef ] [ Medline ]
- Canadian Institute for Health Information (CIHI). Depression Among Seniors in Residential Care. Toronto, ON. Canadian Institute for Health Information (CIHI); 2010.
- Morris JN, Fries BE, Morris SA. Scaling ADLs within the MDS. J Gerontol A Biol Sci Med Sci. 1999;54(11):M546-M553. [ CrossRef ] [ Medline ]
- Morris JN, Fries BE, Mehr DR, Hawes C, Phillips C, Mor V, et al. MDS Cognitive Performance Scale. J Gerontol. 1994;49(4):M174-M182. [ CrossRef ] [ Medline ]
- Matheson FI, Dunn JR, Smith KLW, Moineddin R, Glazier RH. Development of the Canadian marginalization index: a new tool for the study of inequality. Can J Public Health. 2012;103(8 Suppl 2):S12-S16. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Statistics Canada. The Canadian Index of Multiple Deprivation: User Guide. Ottawa, Ontario. Statistics Canada URL: https://www150.statcan.gc.ca/n1/pub/45-20-0001/452000012019002-eng.htm [accessed 2024-02-09]
- Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46(3):399-424. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Perlman CM, Hirdes JP. The aggressive behavior scale: a new scale to measure aggression based on the minimum data set. J Am Geriatr Soc. 2008;56(12):2298-2303. [ CrossRef ] [ Medline ]
- Greenland S, Morgenstern H. Matching and efficiency in cohort studies. Am J Epidemiol. 1990;131(1):151-159. [ CrossRef ] [ Medline ]
- Mansournia MA, Hernán MA, Greenland S. Matched designs and causal diagrams. Int J Epidemiol. 2013;42(3):860-869. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Sjölander A, Greenland S. Ignoring the matching variables in cohort studies—when is it valid and why? Stat Med. 2013;32(27):4696-4708. [ CrossRef ] [ Medline ]
- Stroup WW. Generalized Linear Mixed Models: Modern Concepts, Methods and Applications. Abingdon, England. Taylor and Francis; 2013.
- Suissa S, Henry D, Caetano P, Dormuth CR, Ernst P, Hemmelgarn B, et al. Canadian Network for Observational Drug Effect Studies (CNODES). CNODES: the Canadian network for observational drug effect studies. Open Med. 2012;6(4):e134-e140. [ FREE Full text ] [ Medline ]
- Rosenbaum PR. Observational Studies. New York, NY. Springer; 2002.
- Rosenbaum PR, Rubin DB. Constructing a control group using multivariate matched sampling methods that incorporate the propensity score. Am Statistician. 2012;39(1):33-38. [ CrossRef ]
- Austin PC. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm Stat. 2011;10(2):150-161. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Groll A, Hastie T, Tutz G. Selection of effects in Cox frailty models by regularization methods. Biometrics. 2017;73(3):846-856. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Regional health authorities in Manitoba. Province of Manitoba—Health. Manitoba Health. URL: https://www.gov.mb.ca/health/rha/index.html [accessed 2024-02-11]
- AHS in my zone. Alberta Health Services. 2024. URL: https://www.albertahealthservices.ca/zones/zones.aspx [accessed 2024-02-11]
- Regional health authorities—Province of British Columbia. Ministry of Health, British Columbia. 2024. URL: https://www2.gov.bc.ca/gov/content/health/about-bc-s-health-care-system/partners/health-authorities/regional-health-authorities [accessed 2024-02-11]
- Bronskill SE, Maclagan LC, Maxwell CJ, Iaboni A, Jaakkimainen RL, Marras C, et al. Trends in health service use for Canadian adults with dementia and parkinson disease during the first wave of the COVID-19 pandemic. JAMA Health Forum. 2022;3(1):e214599. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Campbell M, Stewart T, Brunkert T, Campbell-Enns H, Gruneir A, Halas G, et al. Prioritizing supports and services to help older adults age in place: a delphi study comparing the perspectives of family/friend care partners and healthcare stakeholders. PLoS One. 2021;16(11):e0259387. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Harder WP, Gornick JC, Burt MR. Adult day care: substitute or supplement? Milbank Q. 1986;64(3):414-441. [ Medline ]
- Gaugler JE, Zarit SH. The effectiveness of adult day services for disabled older people. J Aging Soc Policy. 2001;12(2):23-47. [ CrossRef ] [ Medline ]
- Alberta SPOR SUPPORT Unit (AbSPORU). URL: https://absporu.ca/ [accessed 2024-08-20]
- Population Data BC. URL: https://www.popdata.bc.ca/ [accessed 2024-08-20]
- Shared Health Research and Innovation. Shared Health Manitoba. URL: https://healthproviders.sharedhealthmb.ca/services/research-and-innovation/ [accessed 2024-08-20]
Abbreviations
| Activities of Daily Living Hierarchy Scale |
| Cognitive Performance Scale |
| discharge abstract database |
| general estimating equation |
| integrated knowledge translation |
| latent class analysis |
| National Ambulatory Care Report System |
| nursing home |
| Resident Assessment Instrument—Home Care |
| REporting of studies Conducted using Observational Routinely-collected health Data |
| Strengthening the Reporting of Observational Studies in Epidemiology |
Edited by T Leung; submitted 02.06.24; peer-reviewed by D Weizhen; comments to author 04.07.24; revised version received 05.07.24; accepted 29.07.24; published 30.08.24.
©Matthias Hoben, Colleen J Maxwell, Andrea Ubell, Malcolm B Doupe, Zahra Goodarzi, Saleema Allana, Ron Beleno, Whitney Berta, Jennifer Bethell, Tamara Daly, Liane Ginsburg, Atiqur SM - Rahman, Hung Nguyen, Kaitlyn Tate, Kimberlyn McGrail. Originally published in JMIR Research Protocols (https://www.researchprotocols.org), 30.08.2024.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work, first published in JMIR Research Protocols, is properly cited. The complete bibliographic information, a link to the original publication on https://www.researchprotocols.org, as well as this copyright and license information must be included.

- Zagazig University
What are the differences between interlaminar and translaminar fracture toughness?
Get help with your research
Join ResearchGate to ask questions, get input, and advance your work.
All Answers (1)

Top contributors to discussions in this field

- University of California, Berkeley

- Xi'an Jiaotong-Liverpool University

- King Abdulaziz University

- Mustansiriyah University

- Natl Scientific & Technical Res Council (CONICET), Buenos Aires; Rosario Natl University, Rosario, Argentina
Similar questions and discussions
- Asked 25 August 2024

- Asked 16 June 2024

- Asked 7 April 2024

- Asked 22 August 2024

- Asked 17 August 2024

- Asked 12 August 2024

- Asked 5 August 2024

- Asked 3 August 2024
- Asked 30 July 2024

Related Publications

- Recruit researchers
- Join for free
- Login Email Tip: Most researchers use their institutional email address as their ResearchGate login Password Forgot password? Keep me logged in Log in or Continue with Google Welcome back! Please log in. Email · Hint Tip: Most researchers use their institutional email address as their ResearchGate login Password Forgot password? Keep me logged in Log in or Continue with Google No account? Sign up
This paper is in the following e-collection/theme issue:
Published on 30.8.2024 in Vol 10 (2024)
Changes in Infectious Disease–Specific Health Literacy in the Post–COVID-19 Pandemic Period: Two-Round Cross-Sectional Survey Study
Authors of this article:
- Yusui Zhao, MD ;
- Yue Xu, MD ;
- Dingming Yao, MD ;
- Qingqing Wu, MD ;
- Heni Chen, MD ;
- Xiujing Hu, MD ;
- Yu Huang, MD ;
Xuehai Zhang, MD
Zhejiang Provincial Center for Disease Control and Prevention, Hangzhou, China
Corresponding Author:
Background: Infectious disease–specific health literacy (IDSHL) is a crucial factor in the development of infectious diseases. It plays a significant role not only in mitigating the resurgence of infectious diseases but also in effectively averting the emergence of novel infections such as COVID-19. During the 3 years of the COVID-19 pandemic, China primarily adopted nonpharmaceutical interventions, advocating for people to avoid crowded places and wear masks to prevent the spread of COVID-19. Consequently, there has been a dearth of research concerning IDSHL and its corresponding focal points for health education.
Objective: This study aimed to (1) evaluate the changes in IDSHL scores between 2019 (before the COVID-19 pandemic) and 2022 (the postepidemic period of COVID-19) and (2) explore the risk factors affecting IDSHL using a multivariate logistic regression analysis.
Methods: This study used 2-round cross-sectional surveys, conducted in 2019 and 2022, respectively, in 30 counties in Zhejiang Province, China. Multiple-stage stratified random sampling was used to select households, and a Kish grid was used to identify participants. An identical standardized questionnaire consisting of 12 closed-ended questions was used to measure IDSHL scores before and after the COVID-19 pandemic (2019 and 2022). Standard descriptive statistics, chi-square tests, t tests, and multivariate logistic regression analyses were used to analyze the data.
Results: The 2-round cross-sectional surveys conducted in 2019 and 2022 yielded, out of 19,366 and 19,221 total questionnaires, 19,257 (99.44% response rate) and 18,857 (98.11% response rate) valid questionnaires, respectively. The correct response rate for the respiratory infectious diseases question “When coughing or sneezing, which of the following is correct?” increased from 29.10% in 2019 to 37.92% in 2022 ( χ ² 1 =332.625; P <.001). The correct response rate for the nonrespiratory infectious diseases question “In which of the following ways can hepatitis B be transmitted to others?” decreased from 64.28% to 59.67% ( χ ² 1 =86.059; P <.001). In terms of IDSHL scores, a comparison between 2022 and 2019 revealed notable statistical differences in the overall scores ( t 1 =10.829; P <.001) and across the 3 dimensions of knowledge ( t 1 =8.840; P <.001), behavior ( t 1 =16.170; P <.001), and skills ( t 1 =9.115; P <.001). With regard to the questions, all but 4 exhibited statistical differences ( P <.001). Multivariate logistic regression analyses indicated that the 2022 year group had a higher likelihood of possessing acquired IDSHL than the 2019 group (odds ratio 1.323, 95% CI 1.264‐1.385; P <.001).
Conclusions: When conducting health education, it is imperative to enhance efforts in nonrespiratory infectious disease health education, as well as respiratory infectious diseases such as COVID-19. Health education interventions should prioritize ethnic minority populations with a poor self-health status and low education.
Introduction
In the final months of 2019, a contagious disease caused by SARS-CoV-2 was discovered in Wuhan, China, and rapidly spread throughout the country and then globally [ 1 ]. From the end of 2019 to the end of 2022, China went through 4 stages [ 2 , 3 ]. The first stage was an emergency response and blockage stage (from the initial outbreak to March 2020). It took approximately 3 months to achieve decisive results in the defense of Wuhan, successfully blocking the domestic transmission of the disease. The second stage consisted of exploring routine prevention and control measures (April 2020 to July 2021). This stage focused on expanding prevention and control measures through nucleic acid testing, controlling the disease within 2 or 3 incubation periods. The third stage was the “dynamic zero” stage of comprehensive and precise prevention and control along the entire chain (August 2021 to February 2022). The goal of this stage was to minimize the occurrence of the disease, efficiently handle scattered cases and clusters, and control the disease within 1 incubation period (14 days) by attempting to achieve the greatest prevention and control effect at the smallest social cost. The fourth stage was the comprehensive prevention and control stage of “scientific precision, dynamic zero” (March 2022 to December 2022). During this stage, in addition to emphasizing rapid and precise prevention and control, comprehensive prevention and control measures were emphasized, including the management of infectious sources, rapid blocking of transmission routes, and protection of susceptible populations. These measures were effectively combined and stacked to prevent the spread of the disease. With the occurrence of viral mutations, changes in the epidemic, access to vaccinations, and the accumulation of prevention and control experience and capabilities, China’s prevention and control of the epidemic entered a new stage—on January 8, 2023, that is, 3 years after China’s COVID-19 epidemic prevention and control campaign began, COVID-19 entered the fifth stage, that is, management [ 4 ]. China had thus entered the post–COVID-19 era.
Research indicated that the application of vaccines has notably diminished the prevalence of COVID-19 infections within the population to a measurable degree [ 5 ]. Apart from vaccinations, nonpharmacological interventions (NPIs) were the most important measures to prevent the spread of the COVID-19 pandemic [ 6 - 10 ], such as maintaining social distancing, wearing masks, washing hands frequently, airing rooms frequently, and taking care when sneezing. The pervasive implementation of vaccines and NPIs was intrinsically linked to public cognition. Only when individuals possessed infectious disease–specific health literacy (IDSHL) and had a comprehensive understanding of COVID-19 did they proactively seek vaccination or adopt NPIs to prevent infection. Consequently, this heightened awareness empowered individuals to actively pursue vaccination or adopt NPIs as strategies to prevent infection of COVID-19 [ 11 ]. IDSHL emphasized 3 key components—cognition, decision-making abilities, and self-efficacy, all of which are essential for the prevention and treatment of infectious diseases [ 12 ]. Since the outbreak of the pandemic, the National Health Commission of China has updated and published its “Novel Coronavirus Infection Prevention and Control Protocol” 10 times [ 11 ], emphasizing that “everyone is responsible for their own health” and for maintaining good hygiene habits such as frequent hand washing, the wearing of masks, strengthening of personal protection, and ongoing promotion of education and awareness. IDSHL and NPIs have indeed played a positive role in effectively preventing COVID-19 infections among Chinese residents. The COVID-19 pandemic has been effectively controlled in China, and the incidence of respiratory and gastrointestinal diseases has significantly decreased [ 6 , 13 ]. This has led to feelings of both satisfaction and concern. In the post–COVID-19 era, when the country no longer requires the public to wear masks and maintain social distancing, it remains to be seen whether the incidence of respiratory and gastrointestinal diseases will continue its downward trend.
Zhejiang, a province in southeastern China, had a population of 64 million at the end of 2020. As a large province, it has seen the second-largest influx of migrant workers in China. These individuals relocated from their homes and now reside in cramped living conditions with inadequate sanitation. They lack many basic rights, such as open access to employment opportunities, free education, social welfare programs, and medical benefits. These conditions significantly increase the risk of outbreaks of infectious diseases. IDSHL is an important determinant of such outbreaks [ 14 ]. The lower an individual’s level of IDSHL, the more likely they are to contract a disease and experience poorer outcomes [ 15 , 16 ]. This suggests that measuring the changes in IDSHL before and after the pandemic may make it possible to predict, with some accuracy, any future changes in the incidence of respiratory and gastrointestinal diseases among residents. However, few studies have explored how IDSHL has changed since the pandemic.
Therefore, the purpose of this study was to (1) evaluate the changes IDSHL scores between 2019 (before the COVID-19 pandemic) and 2022 (the postepidemic period of COVID-19) and (2) explore the risk factors affecting IDSHL among residents using a multivariate logistic regression analysis.
Study Design
This study used 2 cross-sectional surveys, conducted in 2019 and 2022, respectively, in 30 counties in Zhejiang Province, China.
Ethical Considerations
This study adhered to the principles of the Declaration of Helsinki. Informed consent was obtained from all participants or their legal guardians, and all survey responses were collected anonymously. In appreciation of their participation, all participants were presented with a modest gift valued at 50 RMB (about US $7) upon the conclusion of the survey. This study was approved by the ethics committee of the Zhejiang Provincial Center for Disease Control and Prevention (2022-027-01).
Sampling and Recruitment Procedure
The sample size for each county was calculated using the formula:
N = μ α 2 × p ( 1 − p ) δ 2 × d e f f
where α (.05) represents the significance level, µ α (1.96) is the α-quantile of the standard normal distribution, p (26.24%, based on the health literacy level of Zhejiang Province residents in 2018) is the health literacy level, δ (0.03936) is the maximum permissible error, and deff (1) is the design effect of complex sampling. Following the exclusion of invalid questionnaires and rejections (25%), the final sample size for each county was 640. The total sample size of the 30 counties was 19,200. The same sampling method and recruitment procedures were used for both cross-sectional surveys. Multiple-stage stratified random sampling was used to select the participants. Based on the hierarchical administrative system and 2010 Chinese Census data, sampling recruitment procedures were conducted in five stages: (1) 30 counties were selected from the 90 counties in Zhejiang Province, (2) 4 townships were selected within each county, (3) 2 segments (residential blocks) were selected within each township, (4) 100 households were selected within each segment based on a complete list of the addresses of all households, and (5) 1 participant was selected from each household using a Kish grid. Once the ultimate sample outcomes were ascertained, the subsequent recruitment and investigation of participants were exclusively executed by community workers or community health physicians (investigators). First, they contacted the sampled household head by phone, informed them of the family member to be surveyed, and then scheduled a face-to-face visit. If the appointment failed, another one was scheduled. If 3 consecutive attempts to schedule a successful visit failed or recruitment was unsuccessful, we proceeded with the survey by moving on to the next household on the sampling list, and recruitment was restarted. The sampling frame was derived from the 2010 Chinese Census data and field mapping. The eligibility criteria were (1) aged 15‐69 years, (2) able to read or communicate, and (3) accessible to the researchers.
A battery of instruments was used to measure the participants’ IDSHL and collect sociodemographic data ( Multimedia Appendix 1 ). IDSHL was assessed using a subscale of the health literacy surveillance survey questionnaire developed by the National Health Commission of China [ 17 ]. The subscale addresses the knowledge, behavior, and skills related to infectious disease prevention and control. It consists of one true or false item, 8 single-choice items, and 3 multiple-choice items. Each correct response to a multiple-choice question receives 2 points, with 1 point for each correct response to a single-choice or judgment question. The total score for the questionnaire is 15 points. If the respondents scored 12 points or higher, we assumed that they had acquired IDSHL. This subscale is reliable and widely used in China [ 18 ]. Each of the 12 items had a content validity index >0.8, and the overall Cronbach α coefficient was 0.67.
We also collected participants’ sociodemographic data including their sex, age, ethnicity, education, marital status, occupation, and self-health status. A 5-point Likert-type scale was used to assess self-health status (1=excellent, 2=very good, 3=good, 4=fair, and 5=poor).
Data Analysis
Statistical analyses were performed using SPSS (version 18.0; IBM Corp). The mean (SD) and frequency were calculated to describe the quantitative and qualitative variables, respectively. Chi-square tests were used to determine the statistical differences in the demographic characteristics and in each item relating to infectious diseases between the 2019 and 2022 groups. 2-tailed t tests (Welch F test) were used to determine the differences in demographic characteristics and the 3 dimensions of the IDSHL score between the 2 groups. Logistic regression analysis was used to explore the risk factors affecting IDSHL among the participants. A score of P <.05 was considered statistically significant.
The independent variables that were included in all models are sex (male=0 and female=1); age, in years (18‐29=1, 30‐39=2, 40‐49=3, and 50‐69=4); ethnicity (Han=1 and minority=2); education (primary school or lower=1, middle school=2, high school=3, technical school or college=4, and undergraduate or higher=5); marital status (unmarried, divorced, or widowed=0 and married=1); occupation (farmers=1, workers=2, agency or institutional personnel=3, students=4, and other=5); self-health status (excellent=1, very good=2, good=3, fair=4, and poor=5); and year (2019=1 and 2022=2).
Sociodemographic Characteristics of the Groups
A total of 19,366 individuals were surveyed in 2019, with 19,257 valid questionnaires (response rate: 19,257/19,366, 99.44%), and 19,221 individuals were surveyed in 2022, with 18,857 valid questionnaires (response rate: 18,857/19,221, 98.11%). Table 1 presents a comparison of the demographic and health-related characteristics between the 2 groups surveyed in 2019 (n=19,257) and 2022 (n=18,857). There were no statistically significant differences in ethnicity or marital status between the 2 groups, with the vast majority of individuals identifying as Han Chinese (98.93% in 2019 and 98.82% in 2022; P =.32) and married (83.31% in 2019 and 83.23% in 2022; P =.84). However, there were statistically significant differences between the 2019 and 2022 groups with regard to sex ( P =.02), age ( P <.001), education ( P <.001), occupation ( P <.001), and self-health status ( P <.001; Table 1 ). Given the disparities in certain sociodemographic characteristics between the 2 groups, particularly factors such as age and education, which substantially influence IDSHL, there was a potential for the outcomes of the 2 groups to be noncomparable. To ensure the comparability of the results, we standardized both groups using age and education based on the entire surveyed population (N=38,114).
| Content and group | 2019 group (n=19,257), n (%) | 2022 group (n=18,857), n (%) | Chi-square ( ) | value | |
| 5.3 (1) | .02 | ||||
| Male | 9175 (47.65) | 8762 (46.47) | |||
| Female | 10,082 (52.35) | 10,095 (53.53) | |||
| 144.6 (3) | <.001 | ||||
| 18‐29 | 1370 (7.23) | 1529 (8.26) | |||
| 30‐39 | 2313 (12.21) | 2626 (14.19) | |||
| 40‐49 | 2749 (14.51) | 3218 (17.39) | |||
| 50‐69 | 12,513 (66.05) | 11,130 (60.15) | |||
| 1.0 (1) | .32 | ||||
| Han | 19,050 (98.93) | 18,634 (98.82) | |||
| Minority | 207 (1.07) | 223 (1.18) | |||
| 167.9 (4) | <.001 | ||||
| Primary school or lower | 7020 (36.45) | 5887 (31.22) | |||
| Middle school | 6196 (32.18) | 6254 (33.17) | |||
| High school | 3130 (16.25) | 3134 (16.62) | |||
| Technical school or college | 2848 (14.79) | 3480 (18.45) | |||
| Undergraduate or higher | 63 (0.33) | 102 (0.54) | |||
| 0.1 (1) | .84 | ||||
| Unmarried, divorced, or widowed | 3214 (16.69) | 3162 (16.77) | |||
| Married | 16,043 (83.31) | 15,695 (83.23) | |||
| 186.7 (4) | <.001 | ||||
| Farmers | 8738 (45.38) | 7600 (40.3) | |||
| Workers | 2581 (13.4) | 2681 (14.22) | |||
| Agency or institutional personnel | 1927 (10.01) | 1945 (10.31) | |||
| Students | 671 (3.48) | 442 (2.34) | |||
| Other | 5340 (27.73) | 6189 (32.82) | |||
| 40.8 (4) | <.001 | ||||
| Poor | 244 (1.27) | 175 (0.93) | |||
| Fair | 815 (4.23) | 644 (3.42) | |||
| Good | 6242 (32.41) | 5906 (31.32) | |||
| Very good | 5823 (30.24) | 5773 (30.61) | |||
| Excellent | 6133 (31.85) | 6359 (33.72) | |||
| Total | 19,257 (100) | 18,857 (100) | — | — | |
a “Agency or institutional personnel” refers to people working in state organizations, state-owned enterprises, institutions, and other public roles.
b The “Other” category includes unemployed people and those with occupations other than those already listed.
c “Self-health status” refers to respondents’ perceived health status in the preceding 12 months.
d Not applicable.
Comparison of Correct Response Rates for Specific Questions
The data indicated that, in general, the percentage of correct answers increased from 2019 to 2022 for most questions. The single-choice questions saw a statistically significant increase in the percentage of individuals who answered correctly in 2022 compared with 2019 for 3 out of the 8 questions ( P <.001). The multiple-choice questions saw a significant increase in the percentage of individuals who answered correctly in 2022 compared with 2019 for all 3 questions ( P <.001; Table 2 ).
| Types and question | Answered correctly (2019), n (%) | Answered correctly (2022), n (%) | Chi-square ( ) | value | |
| The best way to prevent flu is to take antibiotics (anti-inflammatories). | 10,880 (57.06) | 10,793 (56.66) | 0.6 (1) | .43 | |
| In which of the following ways can hepatitis B be transmitted to others? | 12,257 (64.28) | 11,366 (59.67) | 86.1 (1) | <.001 | |
| For the treatment of tuberculosis patients, which of the following statements is correct? | 12,126 (63.59) | 12,088 (63.46) | 0.1 (1) | .78 | |
| In which of the following situations should vaccination of children be suspended? | 15,514 (81.36) | 15,977 (83.87) | 41.9 (1) | <.001 | |
| If you have a fever, which of the following is correct? | 15,031 (78.83) | 15,811 (83.01) | 107.5 (1) | <.001 | |
| If a virulent infectious disease occurs in a certain place, which of the following practices is correct? | 15,800 (82.86) | 16,502 (86.63) | 104.6 (1) | <.001 | |
| Open windows frequently for ventilation during flu season. Regarding window ventilation, which of the following statements is correct? | 14,117 (74.04) | 14,061 (73.82) | 0.2 (1) | .63 | |
| What is the correct way to read body temperature with a glass thermometer? | 10,115 (53.05) | 10,576 (55.52) | 23.5 (1) | <.001 | |
| If you are bitten by a dog but not seriously, what is the right thing to do? | 18,509 (97.07) | 18,474 (96.99) | .2 (1) | .64 | |
| What should parents do when their children have symptoms such as fever and a rash? | 13,099 (68.70) | 13,673 (71.78) | 43.4 (1) | <.001 | |
| When sick and dead livestock are found, which of the following practices is correct? | 14,818 (77.71) | 15,185 (79.72) | 22.9 (1) | <.001 | |
| When coughing or sneezing, which of the following is correct? | 5549 (29.10) | 7223 (37.92) | 332.6 (1) | <.001 | |
a IDSHL: infectious disease–specific health literacy.
Comparison of IDSHL Scores by Sociodemographic Characteristics
Both males and females showed statistically significant improvements ( P <.001) in scores. All age groups also showed statistically significant improvements ( P <.001) with the youngest age group (18-29 years) having the highest scores in both years. The Han group showed a significant improvement in IDSHL scores ( P <.001), whereas there was no significant change for ethnic minority groups ( P =.95). Education level was also a statistically significant factor, with higher levels of education being associated with greater improvements in IDSHL scores ( P <.001) for all groups except primary school or lower ( P =.08).
Marital status and occupation were also associated with IDSHL score improvements. Unmarried, divorced, or widowed participants and those in certain occupations (agency or institutional personnel, students, and others) showed statistically significant improvements in their IDSHL scores ( P <.001). By contrast, there was no statistically significant change in IDSHL scores for those who reported poor, fair, and good self-health status ( P =.995, P =.094, and P =.03, respectively), whereas participants with very good and excellent self-health status showed statistically significant improvements ( P <.001 for all; Table 3 ).
| Content and group | 2019 survey group (n=19,257), mean (SD) | 2022 survey group (n=18,857), mean (SD) | test ( ) | value | |
| Male | 10.04 (3.13) | 10.37 (3.16) | 7.145 (1) | <.001 | |
| Female | 10.03 (3.19) | 10.40 (3.24) | 8.136 (1) | <.001 | |
| 18‐29 | 11.61 (2.55) | 12.23 (2.35) | 6.808 (1) | <.001 | |
| 30‐39 | 11.51 (2.69) | 12.16 (2.47) | 8.796 (1) | <.001 | |
| 40‐49 | 10.85 (2.93) | 11.26 (2.86) | 5.565 (1) | <.001 | |
| 50‐69 | 9.28 (3.15) | 9.52 (3.20) | 5.813 (1) | <.001 | |
| Han | 10.04 (3.16) | 10.39 (3.20) | 10.845 (1) | <.001 | |
| Minority | 8.87 (2.59) | 8.96 (4.75) | 0.066 (1) | .95 | |
| Primary school or lower | 8.60 (3.09) | 8.69 (3.19) | 1.743 (1) | .08 | |
| Middle school | 9.88 (3.08) | 10.33 (2.97) | 8.180 (1) | <.001 | |
| High school | 11.04 (2.66) | 11.57 (2.61) | 7.967 (1) | <.001 | |
| Technical school or college | 12.19 (2.24) | 12.70 (2.03) | 9.516 (1) | <.001 | |
| Undergraduate or higher | 12.15 (2.29) | 12.98 (1.65) | 2.701 (1) | .01 | |
| Unmarried, divorced, or widowed | 11.06 (2.98) | 11.58 (2.88) | 5.279 (1) | <.001 | |
| Married | 9.98 (3.15) | 10.33 (3.19) | 9.958 (1) | <.001 | |
| Farmers | 9.19 (3.16) | 9.33 (3.28) | 2.739 (1) | .01 | |
| Workers | 9.81 (3.11) | 10.18 (3.07) | 4.263 (1) | <.001 | |
| Agency or institutional personnel | 11.49 (2.72) | 12.35 (2.39) | 10.477 (1) | <.001 | |
| Students | 11.50 (2.57) | 12.11 (2.35) | 4.000 (1) | <.001 | |
| Other | 10.69 (3.01) | 11.14 (2.88) | 8.252 (1) | <.001 | |
| Poor | 8.01 (3.27) | 8.01 (3.15) | 0.006 (1) | .995 | |
| Fair | 9.00 (3.28) | 9.29 (3.33) | 1.678 (1) | .10 | |
| Good | 9.87 (3.07) | 9.93 (3.26) | 1.100 (1) | .30 | |
| Very good | 10.52 (3.11) | 10.96 (3.01) | 7.717 (1) | <.001 | |
| Excellent | 9.94 (3.20) | 10.48 (3.18) | 9.585 (1) | <.001 | |
Comparison of IDSHL Scores for 3 Dimensions
Table 4 presents data related to the health knowledge, behavior, and skills dimensions for the 2-year groups. The results show a statistically significant improvement in the mean scores for all the 3 dimensions between 2019 and 2022. The knowledge dimension showed a statistically significant increase ( P <.001), with mean scores of 4.22 (SD 1.60) in 2019 and 4.43 (SD 1.60) in 2022. The behavioral dimension also showed a statistically significant increase ( P <.001), with mean scores of 4.46 (SD 1.66) in 2019 and 4.73 (SD 1.69) in 2022. The skills dimension showed a statistically significant increase ( P <.001) with mean scores of 1.36 (SD 0.68) in 2019 and 1.42 (SD 0.66) in 2022 ( Table 4 ).
| Subscale | 2019 group, mean (SD) | 2022 group, mean (SD) | test ( ) | value |
| Knowledge | 4.22 (1.60) | 4.43 (1.60) | 8.840(1) | <.001 |
| Behavior | 4.46 (1.66) | 4.73 (1.69) | 16.170(1) | <.001 |
| Skills | 1.36 (0.68) | 1.42 (0.66) | 9.115(1) | <.001 |
| Overall | 10.03 (3.16) | 10.38 (3.20) | 10.829(1) | <.001 |
Multivariate Logistic Regression Analyses
To estimate the effect sizes of these possible risk factors, we conducted a multivariate logistic regression analysis. Table 5 shows the B, SE, Wald test, P value, and odds ratio (OR; 95% CI) values for the potential risk factors. In the multivariate logistic regression model of acquired IDSHL, sex, age, ethnicity, education, marital status, occupation, self-health status, and year group were identified as risk factors. Education is strongly associated with IDSHL. Middle school (OR 2.155, 95% CI 2.028‐2.290), high school (OR 3.590, 95% CI 3.323‐3.879), technical school or college (OR 7.399, 95% CI 6.727‐8.139), and undergraduate or higher education (OR 12.919, 95% CI 8.400‐19.870) were associated with higher IDSHL scores than a primary school education or lower. Self-health status was strongly associated with IDSHL, with a better self-health status being associated with higher IDSHL. Compared with the 2019 group, the 2022 group was more likely to have acquired IDSHL (OR 1.323, 95% CI 1.264‐1.385).
| Variables | β (SE) | Wald | value | OR (95% CI) | |||
| Male (Reference) | 0.065 (0.024) | 7.500 | .01 | 1.067 (1.019‐1.118) | |||
| 18‐29 (Reference) | N/A | N/A | N/A | N/A | |||
| 30‐39 | −0.047 (0.064) | 0.553 | .46 | 0.954 (0.842‐1.081) | |||
| 40‐49 | −0.052 (0.065) | 0.632 | .43 | 0.949 (0.835‐1.079) | |||
| 50‐69 | −0.528 (0.063) | 69.310 | <.001 | 0.590 (0.521‐0.668) | |||
| Minority (Reference) | 0.249 (0.115) | 4.660 | .03 | 1.283 (1.023‐1.608) | |||
| Primary school or lower (Reference) | N/A | N/A | N/A | N/A | |||
| Middle school | 0.768 (0.031) | 612.469 | <.001 | 2.155 (2.028‐2.290) | |||
| High school | 1.278 (0.039) | 1051.036 | <.001 | 3.590 (3.323‐3.879) | |||
| Technical school or college | 2.001 (0.049) | 1697.265 | <.001 | 7.399 (6.727‐8.139) | |||
| Undergraduate or higher | 2.559 (0.220) | 135.729 | <.001 | 12.919 (8.400‐19.870) | |||
| Unmarried, divorced, or widowed (Reference) | 0.248 (0.038) | 43.362 | <.001 | 1.281 (1.190‐1.379) | |||
| Farmers (Reference) | N/A | N/A | N/A | N/A | |||
| Workers | 0.002 (0.037) | 0.002 | .97 | 1.002 (0.932‐1.076) | |||
| Agency or institutional personnel | 0.23 (0.048) | 23.416 | <.001 | 1.259 (1.147‐1.382) | |||
| Students | 0.228 (0.087) | 6.905 | .01 | 1.256 (1.060‐1.490) | |||
| Other | 0.148 (0.031) | 23.230 | <.001 | 1.160 (1.092‐1.232) | |||
| Poor (Reference) | N/A | N/A | N/A | N/A | |||
| Excellent | 0.628 (0.147) | 18.299 | <.001 | 1.874 (1.406‐2.500) | |||
| Very good | 0.82 (0.147) | 31.145 | <.001 | 2.271 (1.702‐3.029) | |||
| Good | 0.632 (0.147) | 18.565 | <.001 | 1.882 (1.411‐2.509) | |||
| Fair | 0.508 (0.159) | 10.244 | .001 | 1.661 (1.217‐2.267) | |||
| 2019 (Reference) | 0.280 (0.023) | 143.296 | <.001 | 1.323 (1.264‐1.385) | |||
| Constant | −2.658 (0.200) | 176.160 | <.001 | 0.041 (0.025-0.073) | |||
b OR: odds ratio.
c N/A: not applicable.
Principal Findings
In the 21st century, China has faced 2 major challenges in the realm of infectious diseases—the resurgence of previously prevalent diseases [ 19 ] and the emergence of new infectious diseases [ 20 ]. China was among the first countries to detect and respond to the COVID-19 outbreak, implementing a robust infectious disease surveillance system. Leveraging this system, China was able to swiftly and effectively mobilize resources to control the spread of COVID-19, resulting in the successful containment of the epidemic within a relatively brief period [ 21 ]. The full application of the concept of the human destiny community provides useful insights into changes in global public health governance [ 22 ]. In general, efforts have been made to enhance the availability and accessibility of global public health products while concurrently fostering international collaboration, and despite a growing population, the incidence, morbidity, and mortality rates of infectious diseases have decreased since 2000 [ 23 ]. The decline in the incidence, morbidity, and mortality rates of infectious diseases in China can be attributed to the country’s ongoing efforts to enhance its infectious disease surveillance system and to its continuous health education initiatives aimed at promoting healthy lifestyle behaviors and improving the public’s IDSHL. As a social determinant of health [ 24 ], IDSHL is known to affect health behaviors, health outcomes, communication with providers, adherence to treatment regimens, and health care costs. Therefore, improving IDSHL is crucial for effective prevention efforts.
In our study, we described the changes in IDSHL scores over time among residents of Zhejiang Province, China, based on representative 2-time-series survey data before and after the outbreak of the COVID-19 pandemic. Our comparative analysis of the sociodemographic characteristics between the 2 groups revealed that the surveyed population in 2022 exhibited higher educational attainment and relatively younger age than the 2019 group. To address this issue and ensure comparability of results, we performed a standardization of the 2 population groups, adjusting for age and education. In addition, the difference could be ascribed to progress in social and economic development, with the implementation of NPIs contributing substantially to the substantial enhancement of residents’ IDSHL [ 25 ]. IDSHL plays a crucial role in mediating the relationship between background data and preventive behaviors [ 26 ]. Therefore, it is of utmost importance to consider IDSHL when designing public interventions. A crucial factor contributing to the success of China’s response to the COVID-19 pandemic was the implementation of prompt and decisive measures by the Chinese government. In the early stages of the outbreak, China effectively used robust containment strategies, resulting in a significant reduction in the number of confirmed COVID-19 cases [ 27 ]. When localized outbreaks emerged, stringent measures, such as rapid nucleic acid testing and rigorous control over transportation, were swiftly enforced, effectively curtailing the spread of the virus.
NPIs reduced the incidence of non–COVID-19 infectious diseases effectively [ 28 ], particularly respiratory infections during the COVID-19 pandemic [ 29 ]. Analyzing specific questions from our survey, the most significant increase in correct response rates between 2022 and 2019 was observed for the question “When coughing or sneezing, which of the following is correct?” The correct response rate increased for this question from 29.10% to 37.92%. Similarly, notable improvements were seen in the questions “If a virulent infectious disease occurs in a certain place, which of the following practices is correct?” and “If you have a fever, which of the following is correct?” The correct response rates increased from 82.86% and 78.83%, respectively, in 2019, to 86.63% and 83.01%, respectively, in 2022. These findings provide further empirical evidence that aligns with the findings of previous studies. One noteworthy observation is that the correct response rate for the question “In which of the following ways can hepatitis B be transmitted to others?” decreased from 64.28% in 2019 to 59.67% in 2022. This result seems to contradict China’s infectious disease surveillance data [ 30 ]. This apparent contradiction may be explained by the fact that China has placed a greater emphasis on COVID-19 prevention and control in recent years, leading to a relaxation in the promotion of preventive measures for nonrespiratory infectious diseases, such as hepatitis B. Consequently, residents’ knowledge regarding the prevention and control of such diseases has declined. We speculate that the decrease in hepatitis B incidence was a result of the stringent isolation and control measures implemented by the government during the pandemic. These measures inadvertently caused some asymptomatic carriers of hepatitis B, who might have been detected while seeking medical attention for other illnesses, to remain undetected, thereby resulting in a potential underestimation of the incidence of hepatitis B. This provides an important reminder that once the COVID-19 pandemic was over, the incidence of nonrespiratory infectious diseases was not only unlikely to continue decreasing but could in fact see a noticeable increase.
This study compared the IDSHL scores of participants with different demographic characteristics in 2 surveys. The findings revealed a greater disparity in IDSHL between Han and ethnic minority groups over the period. Moreover, the ethnic minority groups’ IDSHL scores did not exhibit significant improvement during the 2 survey periods. These findings, which are consistent with research conducted by Tuohetamu et al [ 31 ], suggest that the observed disparity in IDSHL among ethnic minority groups in Zhejiang Province may be attributable more to their low education and income than to language barriers alone [ 32 ]. Education has emerged as one of the most critical factors affecting IDSHL [ 33 , 34 ]. In this study, participants with a primary school education or lower were found to have the lowest IDSHL scores, and no substantial enhancement in their scores was observed across the 2 survey iterations. Plausible explanations for this phenomenon stem from their constrained cognitive capabilities, limited aptitude for learning, and diminished capacity to absorb new information, leading to poor IDSHL acquisition. This study did not see a significant increase in the IDSHL scores of participants who reported poor, fair, and good self-health from 2019 to 2022, suggesting that health education practitioners should try targeted health intervention measures to improve the IDSHL of residents with relatively poor self-health status [ 35 ].
In the multivariate logistic regression analysis, after adjusting for factors such as sex, age, ethnicity, education, marital status, and self-health status, the year group was found to be one of the influencing factors affecting IDSHL. Considering the IDSHL scores and the rates of correct responses to the questions in both surveys, it is evident that there was a significant improvement in participants’ IDSHL in 2022 compared with 2019, following the 3-year COVID-19 pandemic. This improvement can be primarily attributed to the notable enhancement in residents’ knowledge, behaviors, and skills pertaining to the prevention and management of respiratory infectious diseases [ 6 ]. The decline in knowledge about nonrespiratory infectious diseases, however, suggests that, while it is important to reinforce health education among residents regarding respiratory infectious diseases, it is equally important to enhance health education pertaining to nonrespiratory infectious diseases.
Limitations
This study has some limitations. First, the representativeness of our study population compared with the general Chinese population may have been affected by our sampling strategy. Second, it is important to acknowledge that our study used cross-sectional surveys conducted at 2 different time points, which may have introduced a potential selection bias into our sample. Third, given the cross-sectional nature of this study, it was not possible to determine causation. Therefore, we cannot conclude that IDSHL increased because of the increase in COVID-19. Finally, our research population consisted of permanent residents aged 15‐69 years, and some groups were not included; such groups should be included in subsequent studies.
Conclusions
We observed a significant improvement in participants’ IDSHL in Zhejiang Province after 3 years of the COVID-19 pandemic, especially in terms of knowledge and behaviors related to respiratory infectious disease prevention and control. However, we also noticed a decline in the correct response rates for nonrespiratory infectious diseases, such as hepatitis B. Therefore, we believe it is necessary to strengthen health education efforts for nonrespiratory infectious diseases alongside the ongoing education on COVID-19 and other respiratory infectious diseases. We recommend that a provincial infectious disease surveillance system be fully used to monitor infectious diseases in the province, which will enable further research on the relationship between IDSHL and the occurrence of infectious diseases among residents. In addition, to address health disparities and promote equity, health education interventions should prioritize ethnic minority populations in the province with a relatively poor self-health status and low education.
Acknowledgments
This study was financially supported by the Chinese National Sci-Tech Plan Project and local government.
Data Availability
The data sets generated and analyzed during this study are available from the corresponding author on reasonable request.
Authors' Contributions
XZ conceived the study. XZ and YX participated in the design. YZ and DY collected the data. YZ and DY analyzed and interpreted the data. All authors helped draft, read, and approve the final paper. Generative artificial intelligence was not used for any part of the study.
Conflicts of Interest
None declared.
Questionnaire on Infectious-Disease-Specific Health Literacy.
- Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. Feb 20, 2020;382(8):727-733. [ CrossRef ] [ Medline ]
- Liang WN, Liu M, Liu J, Wang YD, Wu J, Liu X. The dynamic COVID-zero strategy on prevention and control of COVID-19 in China. Zhonghua Yi Xue Za Zhi. Jan 25, 2022;102(4):239-242. [ CrossRef ] [ Medline ]
- Shi T, Zhang X, Meng L, et al. Immediate and long-term changes in infectious diseases in China at the “First-level-response”, “Normalized-control” and “Dynamic-COVID-zero” stages from 2020 to 2022: a multistage interrupted-time-series-analysis. BMC Public Health. Jul 18, 2023;23(1):1381. [ CrossRef ] [ Medline ]
- Notice on issuing the general plan for implementing “category B management” for novel coronavirus infection [Article in Chinese]. Comprehensive Group of the State Council Joint Prevention and Control Mechanism for Novel Coronavirus Infection; 2022. URL: https://www.gov.cn/xinwen/2022-12/27/content_5733672.htm [Accessed 2022-12-27]
- Liu C, Lee J, Ta C, et al. Risk factors associated with SARS-CoV-2 breakthrough infections in fully mRNA-vaccinated individuals: retrospective analysis. JMIR Public Health Surveill. May 24, 2022;8(5):e35311. [ CrossRef ] [ Medline ]
- Zhang W, Wu Y, Wen B, et al. Non-pharmaceutical interventions for COVID-19 reduced the incidence of infectious diseases: a controlled interrupted time-series study. Infect Dis Poverty. Mar 9, 2023;12(1):15. [ CrossRef ] [ Medline ]
- Francis NA, Becque T, Willcox M, et al. Non-pharmaceutical interventions and risk of COVID-19 infection: survey of U.K. public from November 2020 - May 2021. BMC Public Health. Feb 24, 2023;23(1):389. [ CrossRef ] [ Medline ]
- Stype AC, Yaya ME, Osika J. Non-pharmaceutical interventions and COVID-19: do county- and state-level policies predict the spread of COVID-19? J Econ Race Policy. Feb 2023;6(2):126-142. [ CrossRef ] [ Medline ]
- Iezadi S, Gholipour K, Azami-Aghdash S, et al. Effectiveness of non-pharmaceutical public health interventions against COVID-19: a systematic review and meta-analysis. PLoS One. Nov 2021;16(11):e0260371. [ CrossRef ] [ Medline ]
- Rizvi RF, Craig KJT, Hekmat R, et al. Effectiveness of non-pharmaceutical interventions related to social distancing on respiratory viral infectious disease outcomes: a rapid evidence-based review and meta-analysis. SAGE Open Med. Jun 2021;9:20503121211022973. [ CrossRef ] [ Medline ]
- Interpretation of the “guidelines for the prevention and control of novel coronavirus infection 10th edition” [Article in Chinese]. Comprehensive Group of the State Council Joint Prevention and Control Mechanism for Novel Coronavirus Infection; 2023. URL: https://www.gov.cn/xinwen/2023-01/07/content_5735448.htm [Accessed 2023-01-07]
- Tian X, Di Z, Cheng Y, et al. Study on the development of an infectious disease-specific health literacy scale in the Chinese population. BMJ Open. Aug 5, 2016;6(8):e012039. [ CrossRef ] [ Medline ]
- Sun J, Shi Z, Xu H. Non-pharmaceutical interventions used for COVID-19 had a major impact on reducing influenza in China in 2020. J Travel Med. Dec 23, 2020;27(8):taaa064. [ CrossRef ] [ Medline ]
- Zhao Y, Xu S, Zhang X, et al. The effectiveness of improving infectious disease-specific health literacy among residents: WeChat-based health education intervention program. JMIR Form Res. Aug 9, 2023;7:e46841. [ CrossRef ] [ Medline ]
- Baumann KE, Phillips AL, Arya M. Overlap of HIV and low health literacy in the Southern USA. Lancet HIV. Jul 2015;2(7):e269-e270. [ CrossRef ] [ Medline ]
- Marciano L, Camerini AL, Schulz PJ. The role of health literacy in diabetes knowledge, self-care, and glycemic control: a meta-analysis. J Gen Intern Med. Jun 2019;34(6):1007-1017. [ CrossRef ] [ Medline ]
- Xiao X, Xiao J, Yao J, et al. The role of resilience and gender in relation to infectious-disease-specific health literacy and anxiety during the COVID-19 pandemic. Neuropsychiatr Dis Treat. 2020;16:3011-3021. [ CrossRef ] [ Medline ]
- Xiang-gang H, Chang-ning L, Ying-hua L, Li L, Xue-qiong N. Analysis of status and influence factors of health literacy of infectious diseases prevention of the urban and rural residents in China [Article in Chinese]. Chin J Health Educ. 2015;31:112-115. [ CrossRef ]
- Wang L, Zhang H, Ruan Y, et al. Tuberculosis prevalence in China, 1990-2010; a longitudinal analysis of national survey data. Lancet. Jun 14, 2014;383(9934):2057-2064. [ CrossRef ] [ Medline ]
- Andrade CR, Ibiapina Cda C, Champs NS, Toledo Junior AC, Picinin IF. Avian influenza: the threat of the 21st century. J Bras Pneumol. May 2009;35(5):470-479. [ CrossRef ] [ Medline ]
- Shuqiong H, Jing C, Peng Z, et al. Reflection on the management of infectious disease information reporting during the COVID-19 outbreak [Article in Chinese]. J Pub Health Prev Med. 2020;31:1-4. [ CrossRef ]
- Liming L. Reflection and prospects on public health in the post-COVID-19 pandemic era. Chinese Medical Information Gazette. Vol 36. 2021:4.
- Zhang X, Hou F, Qiao Z, et al. Temporal and long-term trend analysis of class C notifiable diseases in China from 2009 to 2014. BMJ Open. Oct 17, 2016;6(10):e011038. [ CrossRef ] [ Medline ]
- Yu S, Zhou M, Liu S, Li Y, Hu Y, Ge H. The burden of infectious disease and changing pattern from in 1990 and 2010, China. Zhonghua Yu Fang Yi Xue Za Zhi. 2015;49:621-624. [ Medline ]
- Qiu Y, Qin H, Ying M, Xu K, Ren J. WeChat-based health education to improve health knowledge in three major infectious diseases among residents: a multicentre case-controlled protocol. BMJ Open. Nov 4, 2020;10(11):e037046. [ CrossRef ] [ Medline ]
- Wang H, Cheong PL, Wu J, Van IK. Health literacy regarding infectious disease predicts COVID-19 preventive behaviors: a pathway analysis. Asia Pac J Public Health. Jul 2021;33(5):523-529. [ CrossRef ] [ Medline ]
- Lai S, Ruktanonchai NW, Zhou L, et al. Effect of non-pharmaceutical interventions for containing the COVID-19 outbreak in China. medRxiv. Preprint posted online on Mar 13, 2020. [ CrossRef ] [ Medline ]
- Tanislav C, Kostev K. Investigation of the prevalence of non-COVID-19 infectious diseases during the COVID-19 pandemic. Public Health. Feb 2022;203:53-57. [ CrossRef ] [ Medline ]
- Hu CY, Tang YW, Su QM, et al. Public health measures during the COVID-19 pandemic reduce the spread of other respiratory infectious diseases. Front Public Health. 2021;9:771638. [ CrossRef ] [ Medline ]
- Chen B, Wang M, Huang X, et al. Changes in incidence of notifiable infectious diseases in China under the prevention and control measures of COVID-19. Front Public Health. 2021;9:728768. [ CrossRef ] [ Medline ]
- Tuohetamu S, Pang M, Nuer X, et al. The knowledge, attitudes and practices on influenza among medical college students in Northwest China. Hum Vaccin Immunother. Jul 3, 2017;13(7):1688-1692. [ CrossRef ] [ Medline ]
- Ren Y, Qian P, Duan Z, Zhao Z, Pan J, Yang M. Disparities in health system input between minority and non-minority counties and their effects on maternal mortality in Sichuan province of Western China. BMC Public Health. Sep 29, 2017;17(1):750. [ CrossRef ] [ Medline ]
- Yang P, Ou Y, Yang H, et al. Research on influencing factors and dimensions of health literacy in different age groups: before and after the COVID-19 era in Chongqing, China. Front Public Health. 2021;9:690525. [ CrossRef ] [ Medline ]
- Li Z, Tian Y, Gong Z, Qian L. Health literacy and regional heterogeneities in China: a population-based study. Front Public Health. May 2021;9:603325. [ CrossRef ] [ Medline ]
- Mei X, Chen G, Zuo Y, Wu Q, Li J, Li Y. Changes in the health literacy of residents aged 15-69 years in central China: a three-round cross-sectional study. Front Public Health. Feb 2023;11:1092892. [ CrossRef ] [ Medline ]
Abbreviations
| infectious disease–specific health literacy |
| nonpharmacological intervention |
| odds ratio |
Edited by Amaryllis Mavragani; submitted 12.09.23; peer-reviewed by Adam Palanica, Sun Jing, Weijing Du; final revised version received 22.06.24; accepted 24.06.24; published 30.08.24.
© Yusui Zhao, Yue Xu, Dingming Yao, Qingqing Wu, Heni Chen, Xiujing Hu, Yu Huang, Xuehai Zhang. Originally published in JMIR Public Health and Surveillance (https://publichealth.jmir.org), 30.8.2024.
This is an open-access article distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/4.0/ ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work, first published in JMIR Public Health and Surveillance, is properly cited. The complete bibliographic information, a link to the original publication on https://publichealth.jmir.org , as well as this copyright and license information must be included.
IMAGES
VIDEO
COMMENTS
Research Aims: Examples. True to the name, research aims usually start with the wording "this research aims to…", "this research seeks to…", and so on. For example: "This research aims to explore employee experiences of digital transformation in retail HR.". "This study sets out to assess the interaction between student ...
Frequently Asked Questions What is the difference between research questions and research objectives? Research questions are broad inquiries that guide the direction of the study, identifying the main problem or area of inquiry. Research objectives, on the other hand, are specific, measurable goals that the research aims to achieve.
Research questions are more general and open-ended, while objectives are specific and measurable. Research questions identify the main problem or area of inquiry, while objectives define the specific outcomes that the researcher is looking to achieve. Research questions help define the study's scope, while objectives help guide the research ...
Key Takeaways. Research objectives are specific, measurable goals that a study aims to achieve, while research questions are broad inquiries guiding the overall direction of the research. Clear definitions of both research objectives and research questions are essential for setting a solid foundation for any research project.
Research question. Interest in a particular topic usually begins the research process, but it is the familiarity with the subject that helps define an appropriate research question for a study. 1 Questions then arise out of a perceived knowledge deficit within a subject area or field of study. 2 Indeed, Haynes suggests that it is important to know "where the boundary between current ...
Research studies have a research question, research hypothesis, and one or more research objectives. A research question is what a study aims to answer, and a research hypothesis is a predictive statement about the relationship between two or more variables, which the study sets out to prove or disprove.
Example: Research objectives. To assess the relationship between sedentary habits and muscle atrophy among the participants. To determine the impact of dietary factors, particularly protein consumption, on the muscular health of the participants. To determine the effect of physical activity on the participants' muscular health.
INTRODUCTION. Scientific research is usually initiated by posing evidenced-based research questions which are then explicitly restated as hypotheses.1,2 The hypotheses provide directions to guide the study, solutions, explanations, and expected results.3,4 Both research questions and hypotheses are essentially formulated based on conventional theories and real-world processes, which allow the ...
As the name suggests, these types of research questions seek to explore the relationships between variables. Here, an example could be something like "What is the relationship between X and Y" or "Does A have an impact on B". As you can see, these types of research questions are interested in understanding how constructs or variables ...
Difference Between Aims and Objectives. Hopefully the above explanations make clear the differences between aims and objectives, but to clarify: The research aim focus on what the research project is intended to achieve; research objectives focus on how the aim will be achieved. Research aims are relatively broad; research objectives are specific.
Aligning research questions and objectives is a critical step in conducting a successful study. This alignment ensures that the research remains focused, relevant, and methodologically sound. By clearly defining and interconnecting research questions and objectives, researchers can enhance the clarity, direction, and impact of their study.
The main difference is that research questions focus on the general purpose or aim of the study whereas research objectives provide specific, measurable, and attainable steps to achieve the research questions. Before we move to the differences, let's understand what are Research Questions and Research Objectives: Research Questions: Research ...
In a qualitative study, inquirers state research questions, not objectives (i.e., specific goals for the research) or hypotheses (i.e., predictions that involve variables and statistical tests). These research questions assume two forms: ... There is no significant difference between the effects of verbal cues, ...
The only difference between research questions and objectives is that research questions are stated in a question form while objectives are stated in a statement form. For an objective to be good, it should be SMART: Specific, Measurable, Achievable, Relevant and Time-bound. The importance of research objectives lies in the fact that they ...
Research questions and research objec tives. The Family Physician 2005;13 (3):25-26. Primary care research is best done in primary care. settings. Its aim is to improve the quality of primary ...
To summarize/highlight their definitions: Research questions "arise out of a perceived knowledge deficit within a subject area or field of study." These may be answered either using literature reviews or primary research. Research hypothesis are the formal ideas one seeks to test. (The linked article focuses on null hypothesis test, Chamberlin ...
The presence of multiple research questions in a study can complicate the design, statistical analysis, and feasibility. It's advisable to focus on a single primary research question for the study. The primary question, clearly stated at the end of a grant proposal's introduction, usually specifies the study population, intervention, and ...
Formulating research aim and objectives in an appropriate manner is one of the most important aspects of your thesis. This is because research aim and objectives determine the scope, depth and the overall direction of the research. Research question is the central question of the study that has to be answered on the basis of research findings.
It is a two different things entirely, the research objectives are the purpose or the intended task plan to be achieve in a project while research question is the process of stating the problem of ...
A research aim is a broad statement indicating the general purpose of your research project. It should appear in your introduction at the end of your problem statement, before your research objectives. Research objectives are more specific than your research aim. They indicate the specific ways you'll address the overarching aim.
Answer: A research problem is a broad issue that you would like to address through your research. It identifies a difficulty, doubt, or an area of concern, in theory or in practice, that requires thought and investigation.
If you enjoyed the video, be sure to leave a like and a comment letting me know why. Research Blog - Researcher's Quest - https://researchersquest.wordpress....
Lastly, a research problem is usually stated at the beginning of a research study, while research questions are developed during the research design phase. The research problem sets the foundation for the study, while research questions are refined and finalized based on the research problem and objectives.
The main difference between research concept and abstract Note: Research concept and abstract are two important academic ones, so there is a specific function in scientific research.
Objective: Our research objectives are to (1) compare patterns of day program use (including nonuse) by province (Alberta, British Columbia, and Manitoba) and time; (2) compare characteristics of older adults by day program use pattern (including nonuse), province, and time; and (3) assess effects of day programs on attendees, compared with a ...
Research methodology is the specific procedures or techniques used to identify, select, process, and analyze information/data about a topic. In a research paper, the research methodology section ...
Infectious diseases experts Stuart Cohen and Dean Blumberg answer questions on the 2024-2025 COVID vaccines and who should get them. ... Research arrow_forward. We believe improving health for all is possible. So, our collaborative research includes clinical, translational and basic science studies. ...
Nevertheless, the similarity in periodontal profile between HIV-infected and non-HIV-infected individuals had already been noticed in the pre-cART era: in a cross-sectional study, Scheutz et al. reported no significant difference in PPD and BOP between both groups, suggesting that both frequency and severity of PD in HIV-infected individuals ...
It occurs to me that it is difficult simply because creep-fatigue is a two parameter problem (rather than a 1 parameter problem). Furthermore, I believe it is because the effect of fatigue is ...
With regard to the questions, all but four exhibited statistical differences (P < .001). Multivariate logistic regression analyses indicated that the 2022 year group had a higher likelihood of possessing acquired IDSHL than the 2019 group (OR = 1.323, 95% CI [1.264-1.385], P < .001).